Showing posts with label cerebral palsy. Show all posts
Showing posts with label cerebral palsy. Show all posts
Tuesday, 31 July 2012
Voluntary Exercises Better Than External Stimuli for Physical Rehabilitation
In the Journal of NeuroEngineering and Rehabilitation, July 2012 edition, Dr.Kyung-Lim Joa of the Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan, South Korea published the results of a study in which rehabilitation was evaluated by using voluntary movements as well as Functional Electrical Stimulation (FES).
Nineteen healthy male subjects were enrolled in the study. The study design included: a-voluntary contraction only, b-functional electrical stimulation (FES)-induced wrist extension only, and c-simultaneous voluntary and FES-induced movement. Brain activation was observed in all three modes.
The activated brain regions (number of voxels) of the MI, SI, cerebellum, and SMA were LARGEST DURING VOLUNTARY CONTRACTION ALONE and smallest during FES alone. SII-activated brain regions were largest during voluntary contraction combined with FES and smallest during FES contraction alone. The brain activation extent (maximum t score) of the MI, SI, and SII was LARGEST DURING VOLUNTARY CONTRACTION ALONE and smallest during FES alone.
The conclusions drawn were that voluntary contraction combined with FES may be more effective for brain activation than FES-only movements for rehabilitation therapy. In addition, voluntary effort is the most important factor in the therapeutic process.
As it is this is another proof that the patient recovering from and undergoing rehabilitation for affected limbs due to Parkinson’s, CP, MS, stroke, brain or spinal injuries amongst other diseases and surgeries should be using physical therapy solutions that encourage the patient to use his own strength and efforts while exercising more than outside stimuli via robots or electrical impulses. Such physical therapy products can be found in the TUTOR system.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been designed for just that type of intensive exercise. Consisting of comforatble and ergonomically designed gloves or braces, The TUTORs improve fine motor, sensory and cognitive impairments through intensive exercises with augmented feedback. The exercises are challenging and motivating and allow for repetitive training tailored to the patient’s own performance. In the case of the HANDTUTOR, for example, the glove has been designed to detect finger and wrist motion and has an open palmar surface to give maximum motor and sensory input. The glove comes in different sizes to allow evaluation and treatment of patients from age 5 and up.
One of the most cost effective rehabilitation devices currently in use in leading U.S. and European hospitals the TUTORs are fully certified by the FDA and CE. They can also be used in the patient’s home via telerehabilitaion. See WWW.MEDITOUCH.CO.IL for more information.
Monday, 30 July 2012
First Use of Hand At Age 12
It has just been reported that Kyril, a 12 year old boy from Latvia can now do anything he wants with his right hand for the first time in his life. Kyril is one of a rare group of children that suffered from Brachial Plexus Palsy, a defect that occurs in one in 3-5,000 births that prevents normal movement of the hand. Most children learn to cope with it and 90 percent of them eventually are fine as the disability passes by 3 months of age. With Kyril it didn’t and he was sent to Israel where Dr. Mark Edelman, a pediatric orthopedist and the head of the pediatric orthopedic department at Rambam Medical Center in Haifa, operated on him and ”rearranged” his wrist and shoulder bone. In addition to that miracle Kyril was able to leave the hospital after only one day as the operation precluded the need for a plastic cast and other treatments.
For others who are not so lucky and are suffering from Cerebral Palsy and other disabling diseases getting the right type of physical therapy solution is critical in order to restore normal movement in the affected limb. Such a solution can be found in the TUTOR system. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been included in physical therapy programs at leading U.S. and European hospitals and rehabilitation facilities. These devices are ergonomically designed gloves and braces that have sensors to detect even the slightest movement on dedicated software they are connected to. The physical therapists then record and quantify this information and design a customized intensive exercise program with augmented feedback leading to enhanced rehabilitation for the patient.
The TUTOR system is suitable for children as well as adults and can be used at the patient’s home through telerehabilitation. The TUTORs are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.

Wednesday, 25 July 2012
Parkinson’s Disease–Not This Population
In the northern part of Israel and in Syria there is a group of people called ”Druse”. A new study by the University of Haifa and the Carmel and Rambam Medical Centers in Israel has found that the Druse people have a much lower incidence of Parkinson’s disease (PD) than in other populations. In addition it was found that this group suffers less from Essential Tremor (ET). This despite that the Druse tend to intramarry, a fact that usually brings with it higher genetic disease rates.
Funded by the Israeli Ministry of Science and Technology the researchers found that the group is a “genetic nature reserve” since they have lived in the same general area for over 1,000 years and do not marry outsiders. Amongst the statistics is the fact that in the rest of the world ET affects an average of 4% of the poulation over 40 and PD an avaerage of 1.5%.
The study was conducted with 9000 Druse who were 51 or over and who live in the Galilee section of Israel. Blood samples were taken from those who suffered from any kind of tremor. Of the group only 27 had full tremors and 9 had PD. The researchers were surprised at the low at the low percentage for a group of people that practiced consanguinity (marrying cousins). Normally such a group would be more likely to get PD and ET. A previous survey, though, discovered that genetically 150 different genealogical lines made up the community. This suggested to the researchers that because of so many lines when the community was originally formed it prevented the increase in genetic diseases.
For those people who are not part of the Druse population Parkinson’s disease can be very debilitating. Fortunately there are physical therapy solutions that can offer some relief for PD symptoms. At the forefront is the HANDTUTOR.
The newly developed HANDTUTOR and its sister devices (LEGTUTOR, ARMTUTOR and 3DTUTOR) have become a key system in neuromuscular rehabilitation and physical therapy for Parkinson’s patients as well as those affected by brain/spinal cord injury and other upper and lower limb disabilities . These innovative devices implement an impairment based program with augmented feedback that encourages intensive practice and motor learning through active exercises. The exercises are challenging and motivating and allow for repetitive and intensive training tailored to the patient’s performance and motor, sensory and cognitive movement ability. Customized and simple but powerful rehabilitation software allows the physical and occupational therapist the ability to adjust the program and exercise difficulty to the patient’s movement level. The system also includes objective quantitative evaluations that allow the physiotherapist and his occupational therapist colleagues to report on the patient’s exercise progress.
Telerehabilitation features allow the patient to be supported by the physical rehabilitation team when he is at home. This ensures that the patient is motivated to do more practice between treatments by the therapists. The TUTOR system is suitable for children as well as adults. They are certified by the FDA and CE and are available for children as well as adults. See WWW.MEDITOUCH.CO.IL for more information.

Tuesday, 17 July 2012
Prehabilitation–a Definition
PREVENTION & REHABILITATION: Two words that are not usually mentioned in the same breath. They actually are at opposite ends of the spectrum. However they really can go together because as much as rehabilitation serves to heal the injured, prevention or ”prehabilitation” can prevent the injury.
To explain it further there are two areas of rehabilitation:
a) Prehabilitation: which is exercise therapy undertaken by athletes and others to try to reduce the risk of injury.
b) Rehabilitation: is exercise therapy which is used to strengthen muscles around limbs and thereby attempt to return the use of an affected limb to its previous healthy state and also to prevent the injury from recurring. This method can be used to build up muscles and reduce injury around the shoulder, arm, leg and other upper and lower limbs of the body. Players of contact sports such as Rugby in the UK or football in the U.S., as an example, can be the beneficiaries of such prehabilitation.
Using the best physical therapy solutions for prehabilitation would add to the success of prevention of severe injuries. Such physical therapy products as the TUTOR system will afford the athlete and others to accomplish the goal of muscle toning and strengthening. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been introduced to provide intensive exercises for disabilities arising from stroke, CP, MS, brain/spinal cord injuries and other upper and lower limb injuries or diseases. The same TUTOR system can be used to exercise various muscles of the body on a regular basis to help prevent injury due to sports and other accidents. The TUTORs are ergonomically designed gloves and braces that are attached to various parts of the body and through powerful evaluation software accessed by sensors in the braces that allow the patient to perform intensive exercises. The exercises are monitored by physical therapists who then design a custom made program appropriate for that patient’s ability level.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are fully certified by the FDA and CE. They are available for children as well as adults and can be used in the patient’s home through telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Sunday, 8 July 2012
Dolphin Assisted Therapy (DAT) and Cerebral Palsy
Dolphins have been used to treat a variety of ailments including autism, cerebral palsy, trauma and cancer among other disabilities.
Dolphin-assisted therapy (DAT), as a part of animal-assisted therapy and complementary and alternative medicine, yields several positive results. A study in the Ukraine called ”Dolphin Swim” used 37 participants who were parents of special needs children. The children suffered from a variety of diagnoses which included emotional and physical disorders. Five treatment programs took place over a span of 2 weeks. A comparison was made with pretreatment and post treatment using DAT (Dolphin Assisted Therapy). The results showed positive behavioral changes in the affected children.
In Israel at the Eilat Dolphin Reef Dr. Ilan Kutz of the Meir Medical Center has supervised the unusual treatment and rehabilitation of trauma victims. DAT is not a cure but alleviates symptoms significantly. Dolphins are very intelligent creatures and have a language of clicks and physical movements. They enjoy communicating with humans and like to be touched, petted and cuddled. The mammals react to the person if they feel a connection to him and then they will give unconditional love. In a particular case of a young man that was severely beaten and even after his physical wounds were healed he didn’t speak. Working with the Dolphins greatly improved his swimming skills and he now speaks normally.
Aside from this unusual therapy the CP patient can hope to improve limb movement ability with the use of the TUTOR system. This most cost effective physical therapy solution (as is the dolphin therapy) is currently used in leading U.S. and European hospitals and clinics. The system which includes the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are ergonomic wearable devices together with powerful dedicated rehabilitation software. The TUTOR system consists of motivating and challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. The physical therapist can then record and design a custom made exercise program for that particular patient’s needs.
The Tutors are also available for adults and children and can be used in the patient’s home through the use of telerehabilitation. They are fully certified by the FDA and CE.
See WWW.MEDITOUCH.CO.IL for more information.

Wednesday, 4 July 2012
Don’t Underestimate Pre Knee/Hip Surgery Exercises
All those that undergo knee or hip replacement surgery need to get into anexercise program following surgery. However it is equally important to have an exercise program prior to these surgeries as well so as to strengthen the muscles around the joint. This will both enhance the recovery and properly support the new joint. How much exercise to do is an individual choice and will depend on a number of factors. If the exercise causes pain it would be better to curtail it. It is preferable to exercise once or twice a day every day before surgery and to do five repetitions of each exercise and then gradually increase them until the actual date of surgery. Doing the exercises in bed lying down is excellent. Your doctor or physical therapist can prescribe specific exercises for your condition.
An excellent plan would be to use the LEGTUTOR as a physical therapy product as it has a reputation for ease and comfort. The LEGTUTOR consists of a safe and comfortable leg brace with position and speed sensors that precisely record 3 dimensional hip and knee movements. The LEGTUTOR has a range of motion limiter that can limit the dynamic range of knee extension and flexion. Rehabilitation games allow the patient to exercise Range of Motion (ROM), speed and accuracy of movement. The LEGTUTOR facilitates evaluation and treatment of the lower extremity including isolated and combined hip and knee movements. The LEGTUTOR together with its sister devices (HANDTUTOR, ARMTUTOR and 3DTUTOR) are currently used successfully in leading U.S. and European hospitals for a variety of disabilities including stroke, CP, MS Brain and Spinal cord injury and others affecting the upper or lower limbs. The TUTOR sytem is available for children as well as adults and are fully certified by the FDA and CE. The TUTORs can also be used at home through telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Thursday, 28 June 2012
Closed and Open Chain Exercises as a Prelude to Knee and Hip surgery
Closed chain exercises are physical exercises performed where the hand (for arm movement) or foot (for leg movement) is fixed in space and cannot move. The extremity remains in constant contact with a stationary surface, usually the ground or the base of a fixed object.
The opposite of closed chain exercises are open chain exercises. Closed chain exercises are considered safer and more “functional” compared to open chain exercises. Nevertheless, the two families of exercises can co-exist in enabling rehabilitation and strengthening objectives.
Closed chain exercises are often compound movements, that generally incur compressive forces, while open-chain exercises are often isolation movements that promote more shearing forces.
Closed chain exercises involve more than one muscle group and joint simultaneously rather than concentrating solely on one, as many open chain exercises do (single-joint movements), lending the former to more utilitarian and athletic activities.
Open Chain Exercises allow the hand or foot freedom to move (like a chest press). These types of movements tend to isolate a single muscle group and a single joint. For example, the one joint involved during a leg extension is the knee and the muscle group it isolates is the quadriceps. Open chain exercises can be done with or without added weight, but when weight is added, it’s usually placed at the distal (far away) portion of the limb (like the ankle). Examples of open chain exercises include chest presses, biceps curls, leg curls, and leg extensions (with or without added weight).
In Closed Chain Exercises the movements of hands or feet are in a constant, fixed position (usually on the ground) during the exercise (such as pushups). Closed chain exercises work multiple joints and multiple muscle groups at once. For example, a squat involves the knee, hip and ankle joints, and multiple muscles groups (quads, hamstrings, hip flexors, calves and glutes). Closed chain exercises can be done with body weight alone or with added weight. When external weight is added, it is usually rested across the back of the shoulders or the front of the chest, which is considered much safer than the “distal” placement of weight during open chain exercises. Examples of closed chain exercises include pushups, pull-ups, squats, and lunges, all of which can be done with or without added weight.
These exercises are useful for several purposes and can either strengthen knee and hip muscles prior to replacement and may even be able to prevent the surgery completely.
When exercising the various muscles it would be very helpful to use the most effective physical therapy products available. Specifically the TUTOR system of products (HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR) have been designed to strengthen and revitalize limb muscles that may have been compromised over time by arthritis, Parkinson’s disease, CP, MS, brain or spinal cord injuries, tendon transfers, complex regional pain syndrome and others.
The TUTOR system consist of ergonomic wearable devices together with powerful dedication rehabilitation software. The system is indicated for patients in rehabiliation centers, private clinics and the home and can be supported by telerehabilitation.
The TUTORs consists of motivating and challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. Controlled exercise practice will help to prevent the devlopment of compensatory movement patterns. The dedicated software allows the therapist to fully customize the exercises to the patient’s movement ability.
The TUTOR system is fully certified by the FDA and CE and is available for children as well as adults.
See WWW.MEDITOUCH.CO.IL for more information.

Wednesday, 27 June 2012
Physical Therapy for Multiple Sclerosis Patients
What role does physical therapy play in treating MS?
Physical therapy can help with
Balance problems
Coordination issues
Fatigue
Pain
Weakness
Difficulty with physically performing daily activities (such as walking or getting up from a sitting position)
Posture
The goal of physical therapy is to improve independence and quality of life by improving movement and function, and relieving pain.
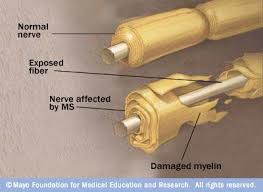
We don’t know why yet but Multiple Sclerosis (MS) damages the myelin sheath surrounding the nerve cells of the brain and spinal cord. Scarring from this damage can block or slow nerve impulses in areas of the brain (neurological damage). As a result, an MS patient may lack coordination, feel tired, have involuntary movements, resist movement (spasticity), and have pain. Symptoms such as these, which are a result of MS, are called “primary symptoms.”
Primary symptoms can reduce movement. As a result, one may feel tightness, pain and weakness, especially in the muscles and joints. These are called “secondary symptoms”.
Physical therapy cannot cure primary symptoms because, at this time, neurological damage cannot be reversed. Physical therapy can be helpful, though, by providing “compensatory” treatments. These treatments enable the patient to compensate for the changes brought about by MS. Compensatory treatments include learning new movement techniques, strategies, and equipment.
Physical therapy can be very helpful at lessening and even stopping secondary symptoms of MS. A physical therapist can teach exercises to be used to strengthen and stretch muscles. Many of these exercises can be performed at home.
A physician can refer the patient for physical therapy if the patient feels there may be benefit from it.
The number of PT appointments depends on the specific situation. The first appointment includes an evaluation and recommendations for exercises. The following appointments check your progress and build a new program. The therapist will work with the patient until a certain level of improved function is reached. At that point, a home exercise program may be developed.
When choosing the right physical therapy solution it is vital to incorporate the best physical therapy products. Such a product is the TUTOR system. Currently being used for the treatment of MS as well as CP, stroke, brain/spinal cord injury, Parkinson’s disease and other upper and lower limb surgeries the TUTORs are amongst the leading medical devices for physical therapy. The TUTORs which consist of the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR consist of comfortable ergonomically designed gloves and braces that are connected to exclusive games that allow the patient to practice isolated and/or interjoint coordination exercises. Controlled exercises prevent the development of compensatory movement patterns. The dedicated software allows the therapist to fully customize the the exercises to the patient’s ability. In addition the therapist can objectively and quantitatively evaluate and report on the treatment progress.
The TUTOR system is available for children as well as adults and in the patient’s home through the use of telerehabilitation.
See WWW.MEDITOUCH.CO.IL for more information.
Tuesday, 26 June 2012
The Knee Ligaments and Their Rehabilitation After Injury
The anterior cruciate ligament (ACL) is one of the four major ligaments of the human knee. When it is injured the doctor or even physical therapist will design a physical rehabilitation (rehab) program that takes into consideration what the normal level of activity is usually like, the state of physical fitness, and the extent of the anterior cruciate ligament (ACL) injury itself.
Such a rehab program should include: flexibility exercises, strengthening exercises, endurance activities and coordination and agility training (for competitive athletes)., The program should function until all of the muscles in the injured leg should be as strong as in the uninjured leg before one returns to normal activities. The program usually includes treatment with a physical therapist at a therapy center, home treatment, at a gym or health club. Generally, the less one sees the therapist, the more one does on his own.
The extent of the recovery from an ACL injury depends on how severe the injury was originally, how extensive the surgery was, and how consistent one is in the follow up program. The rehab program normally lasts from 4 to 6 months. People who are more consistent with their program make a faster recovery and have fewer knee problems in the future than those who do not complete their program.
Rehabilitation is needed after most ACL injuries, regardless as to whether surgery takes place. Rehabilitation programs strengthen the knee and the muscles around it which leads to better knee stability, and may also return normal range of motion and flexibility to the knee. How well a rehab program works depends on whether one does rehab only or has surgery plus a rehab program. It is important to establish what to expect from the rehab program. This depends on age, the extent of your injury, whether other knee injuries are present, and overall health.
In rehab only, some people are able to regain enough stability in their knee to continue their normal activities and are able to avoid surgery. Other people have poor results, never regain knee stability, and either decide to have surgery or quit their activities or sports. If rehabilitation is done without surgery, there is a greater chance that the ACL may be injured a second time., Athletes who have surgery followed by complete rehab are more likely to return to competitive sports than those who only do rehab.
It is vital to have the rehabilitation program well supervised to ensure that the exercises are appropriate and the progression is appropriate. The risks of a speedy rehab program may weaken the reconstructed ligament, and starting sports training too soon. If the rehab program is not completed, there is a risk of having an unstable knee and reinjuring it in the future.
Physical rehabilitation for an ACL injury is extensive. Some people consider it like having a second job., To the extent that one participates in a rehab program, knee surgery may be avoided because strengthening the muscles in the front (quadriceps) and back of the thigh (hamstrings) will support the knee. If surgery is eventually needed though, one will be much better prepared for surgery and rehabilitation after surgery.
It is important to know that not all physical rehabilitation programs are the same. In the field of physical rehabilitation it is important to have access to the best physical therapy solutions in the sense of the most efficient tools that are available. Included in such physical therapy products is the LEGTUTOR. The LEGTUTOR consists of a safe and comfortable leg brace with position and speed sensors that precisely record three dimensional hip and knee movements. The LEGTUTOR has a range of motion limiter that limits the dynamic range of knee extension and flexion. Rehabilitation games allow the patient to exercise range of motion, speed and accuracy movement. The LEGTUTOR facilitates evaluation and treatment of the lower extremity including isolated and combined hip and knee movements.
The TUTOR system (of which the LEGTUTOR is one component, the others being the HANDTUTOR, ARMTUTOR and 3DTUTOR) is one of the most cost effective physical therapy solutions.These physical therapy products are also used for patients with Parkinson’s disease, stroke, brain or spinal cord injury and other upper and lower limb surgery rehabilitation. The TUTOR system is currently in use in leading U.S. and European hospitals and clinics. The TUTOR system is available for children as well as adults and can be used at the patient’s home through terehabilitation. The TUTORs are FDA and CE certified. See WWW.MEDITOUCH.co.il for more information.
Sunday, 24 June 2012
Diabetes Drug for Brain Injury Discovery
On June 24, 2012 it was reported that a new diabetes drug-called Exendin-4 which has been approved by the FDA significantly minimizes damage in Traumatic Brain Injury (TBI) in laboratory animals. The project was commissioned by the U.S. Air Force. The principal researchers are Prof. Chaim Pick of Tel Aviv University’s Sackler Faculty of Medicine and Dr. Niguel Greig of the U. S. National Institute of Aging.
Although the death toll in people who suffer from TBI is relatively low, it can have severe, lifelong consequences for brain function. As a result of TBI a patient can have impaired mental abilities and dramatic personality changes. This aside from the high financial cost of treatment.
Originally Exendin-4 was designed to control sugar levels in the body but it has shown to be effective in alleviating symptoms of Alzheimer’s disease and it was found that if administered shortly after the original incident it can minmize damage in TBI. Together with collaborators, Dr. Vardit Rubovitch, Lital Rachmany-Raber and Prof. Shaul Schreiber and Dr. David Tweedie of the U.S. Institute the study and results have been published in the journal Experimental Neurology.
The research has been going on for several years and consisted of the effects of injuries when hitting the windshield in a car accident as well as work for the U.S. military in relation to trauma sustained when someone is exposed to an explosion or terrorist attack. In the experiments it was shown that mice that were exposed to blasts but that received Exendin-4 had significant reduction of brain damage caused by the explosion. An improved outcome was also associated when the mice sustained TBI by blunt force if given the drug . The plan now is to find the right dosage and delivery system and to find other drugs to complement Exendin-4 to increase its efficiency.
TBI can have debilitating effects on limb movement and when that occurs the best physical therapy solutions are needed to provide exercises for the patient. The most cost effective physical therapy poducts are incorporated into the TUTOR system. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are comfortable ergonomically designed gloves and braces that are placed on strategic locations of the body. They have position and speed sensors that precisely record finger and wrist movement. Rehabilitation games allow the patient to exercise range of motion, speed and accuracy of movement including opposition and pinch movement practice. The software gives the physical therapist objective and quantitative information which then allows an exclusive exercise treatment plan to be designed.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are also used by patients that have impaired limb mobility due to stroke, Parkinson’s, CP,MS, spinal cord injury and other upper and lower surgeries. Currently in use in leading U.S. and European hospitals and clinics the TUTOR system is FDA and CE certified and is available for children as well as adults. The patient is also able to use the TUTORs from home, if necessary, through the use of telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.
Thursday, 21 June 2012
A ”Pacemaker” for Parkinson’s Patients
In line with the international effort to combat symptoms of Parkinson’s disease, it was announced on June 20, 2012 that Professor Hagai Bergman of Jerusalem’s Hebrew University’s neurobiology department had been able to surgically implant a battery operated neurostimulator, similar to a heart pacemaker, to deliver electrical stimulation to specific parts of the brain that control movement. This tiny device blocks the abnormal nerve signals that cause the severe shaking and other symptoms that Parkinson’s patients experience. About 0.4% of the Israeli Parkinson’s population had already received the new device but there was further adjustment necessary.
For Parkinson’s patients that are not acceptable for this procedure and for those that are still waiting for the special surgery other methods are needed to counter the debilitating movements that are prevalent with this disease. When these latter patients are in need of physical therapy solutions the TUTOR system comes in handy. The TUTORs, which consist of the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR, are comfortable ergonomic gloves and braces placed on various limbs of the body and are connected to a computer with dedicated software that allows the patient to get intensive exercises. These exercises are in the form of challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. Controlled exercise practice will help to prevent the development of compensatory movement patterns. The dedicated software allows the therapist to fully customize the exercises to the patient’s movement ability. In addition the the therapist can objectively and quantitatively evaluate and report on treatment progress. The rehabilitation system optimizes the patient’s motor, sensory and cognitive performance and allows the patient to better perform everyday functional tasks to improve their quality of life.
The TUTORs are currently used in leading U.S. and European hospitals and clinics to treat patients that have Parkinson’s disease as well as CP, MS, stroke, brain and spinal cord injury and other upper and lower limb disabilities.
The TUTORs are one of the most cost effective physical therapy tools on the market and are fully certified by the FDA and CE. They are available for adults as well as children and can be used at home via telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.
Wednesday, 20 June 2012
Rehabilitation: What Does it Actually Mean?
Rehabilitation can mean many things to many people. A building that is old and rundown needs to be rehabilitated, a criminal during his imprisonment is hopefully rehabilitated so he can return productively to society, a person accused of some scandal needs to be rehabilitated back into the good graces of the society he came from. Rehabilitation , obviously, also means physical rehabilitation after a severe injury or disease. In the latter situation it isn’t enough for the patient to be hospitalized for a period of time and then return home. There is a very complicated process performed by very highly trained individuals that work as a team to assure that the patient is able to function as close to his normal ability as possible.
Traumatic spinal cord injury (SCI) is perhaps one of the most devastating orthopedic injuries and the primary goals of rehabilitation are: a) prevention of secondary complications, b)maximization of physical functioning, and c)reintegration into the community.
SCI rehabilitation is most effective with a multidisciplinary, team-based approach, as follows:
Physical therapists typically focus on lower extremity function and with mobility functions.
Occupational therapists are involved with upper extremity dysfunction and difficulties in activities of daily living
Rehabilitation nurses are concerned with issues of bowel and bladder dysfunction and managing pressure ulcers
Psychologists deal with emotional and behavioral concerns of the injured patient and with any potential cognitive dysfunction
Speech-language pathologists focus on issues of communication and swallowing
Case managers and social workers are the primary coordinators between the rehabilitation team, the patient and family, and the financial source.
A physiatrist manages the whole team. He is a physician who specializes in physical medicine and rehabilitation. While each team member has primary responsibilities, any other member of the team can contribute to the resolution of any problem.
When it comes to choosing the most appropriate physical therapy tools the team would hopefully consider the most cost effective and efficient devices on the market. Such a tool would be the TUTOR system. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are used extensively in Spinal Cord Injury rehabilitation.
The TUTOR system consists of ergonomic wearable devices together with powerful dedicated rehabilitation software. The system is indicated for patients in rehabilitation centers, private clinics and the home where it can be supported by telerehabilitation. It is designed for those who have head, trunk, upper and lower extremity movement dysfunction.
The system consists of motivating and challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. Controlled exercise practice helps to prevent the development of compensatory movement patterns. The dedicated software allows the therapist to fully customize the exercises to the patient’s movement ability. In addition the therapist can objectively and quantitatively evaluate and report on the treatment progress. The rehabilitation system optimizes the patient’s motor, sensory and cognitive performance and allows the patient to better perform everyday functional tasks to improve their quality of life. The TUTOR system is FDA and CE certified and can be adapted to children as well as adults. See WWW.MEDITOUCH.CO.IL for more information.
Tuesday, 19 June 2012
The Effects of Traumatic Brain Injury on Fatigue and Sleepiness
Simon Beaulieu-Bonneau and Charles M. Morin of the École de psychologie, Université Laval, Pavillon Félix-Antoine Savard 2325, rue des Bibliothèques, Québec, Canada conducted a study comparing individuals who suffered from a traumatic brain injury (TBI) to healthy controls (CTLs) measuring sleepiness,fatigue, and sleep and exploring the relationship between each group.
There were 22 adults with moderate to severe TBI and 22 matched healthy CTLs. They underwent one night of polysomnographic (PSG) recording of their sleep followed the next day by the Maintenance of Wakefulness Test (MWT). They also completed a 14-day sleep diary, the Epworth Sleepiness Scale (ESS), the Functional Outcomes of Sleep Questionnaire (FOSQ), and the Multidimensional Fatigue Inventory (MFI).
The results showed that there were no significant group differences on measures of subjective or objective sleepiness, both groups being quite alert. However, TBI participants reported greater consequences of sleepiness on their general productivity, spent more time in their bed at night, and napped more often and for longer periods of time during the day. Subjective fatigue was significantly higher in TBI participants on the general, physical, and mental fatigue MFI subscales. There were no between-group differences on any sleep parameters derived either from PSG or sleep diary.
The conclusions they reached were that fatigue appeared to be a more prominent symptom than sleepiness when it was assessed between 1 and 11 years after TBI. Patients that participated who suffered from TBI used compensatory strategies such as increasing time spent in bed and napping during the day in this sample.
When TBI causes immobility of a limb the appropriate physical therapy solution should be found. For example the TUTOR system of physical therapy products know as the: HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are used extensively to accomplish the proper exercise program.
Physical rehabilitation is being done in the USA at major rehabiliaiton in-patient and out-patient clinics as well as at private physical therapy clinics. Many patients who have had a TBI or stroke, cerebral palsy or spinal cord injury can also avail themselves of the TUTOR system through the use of tele rehabilitation. These physical therapy products have been developed to allow for functional rehabilitation of the whole body including the upper and lower extremity. The system consists of ergonomic wearable devices and dedicated rehabilitation software that provides patient instructions and feedback to encourage intensive and controlled exercise practice. In this way, the TUTOR system allows for exercise of multijoints within the normal movement pattern which prevents the development of undesired and compensatory joint movement and therefore ensures better performance of functional tasks. This is important in stroke, brain, spinal cord (SCI) and Cerebral palsy rehabilitation in addition to other neurological and orthopedic injury and disease.
Additional features of the TUTOR system include quantitative evaluation and objective follow up that is important in the physiotherapists treatment of the exercises.
For additional information see WWW.MEDITOUCH.CO.IL
Monday, 18 June 2012
Exercise Improves Balance
Bilge Kara and Arzu Genc of Dokuz Eylul University, School of Physical Therapy, Izmir, Turkey and Beril Donmez Colakoglu and Raif Cakmur of the Neurology Department of Faculty of Medicine, Dokuz Eylul University, Izmir, Turkey conducted a study to examine what the effects were of supervised exercises on measures of static and dynamic balance of Parkinson’s disease (PD) patients.
The study used a before/after design. Seventeen PD patients with mild and moderate levels of disability were included in the study. Under a physiotherapist’s supervision patients followed an exercise program once a week for 12 weeks. The standard Balance Master protocol was used before and after exercise to assess changes in static and dynamic balance.
The results showed that there was a statistically significant difference in the unilateral balance test, one of the static balance assessments performed while standing on the right or left leg with closed eyes. With respect to dynamic balance, a statistically significant difference in the maximum excursion of limits of stability (LOS), one of the balance tests used in the exercise programs for patients with Parkinson’s disease, between measurements taken both before and after exercises was also detected.
The conclusions drawn were that the change of LOS revealed that dynamic balance improved due to the exercises. Therefore, the supervised exercise program showed improvement in the dynamic balance of PD patients.
One of the most comprehensive exercise programs available today for PD patients is the one using the TUTOR system as a physical therapy solution.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are being used both inpatient, outpatient and in the home care environment to encourage intensive repetitive exercise practice in a controlled and motivating format. The TUTORs are used in both early intervention by both physical and occupational therapists. In addition the TUTOR system is used to continue to keep the patient motivated and to do exercise practice during the later stages of rehabilitation and to keep the gains that have been achieved in movement and functional ability. The TUTORs are being used in exercise rehabilitation for Parkinson’s patients as well as those who have had a stroke, brain/spinal cord injury, CP, MS and a host of other upper and lower limb disabilities. The patient can start to do intensive repetitive exercises even if they have limited lower limb, shoulder, knee and ankle or upper limb arm and hand movement ability. When it comes to balance therapy the LEGTUTOR and/or 3DTUTOR are placed on either the impaired or non impaired leg while the patient stands and ”throws darts” in one of the many exclusively created games that the TUTOR system uses. This allows the patient to strengthen both legs while working on balance and cognition.
The TUTOR physical therapy products are currently in use in leading U.S. and European hospitals and clinics. They can be used by children as well as adults and at home through the use of telerehabilitation. They are certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.
Sunday, 17 June 2012
The Dangers of Silent Stroke
While the public is generally aware of strokes and their after effects less is known about ”silent strokes”.
Normal symptoms of a stroke are usually obvious, like numbness or weakness on one side of the face, difficulty walking, trouble speaking and vision problems. Some strokes, though, pass completely without being noticed. But even these can have a significant and lasting effect on memory, according to the June 2012 issue of the Harvard Women’s Health Watch.
These so-called ”silent strokes” create points of dead cells in the brain. The damaged areas are smaller than with a traditional stroke. They often don’t affect areas of the brain that are associated with movement or speech.
During an ischemic stroke, a blood clot blocks a blood vessel that feeds part of the brain. If there is no steady supply of blood, cells in that area stop functioning and may die. The symptoms that appear reflect functions that were under the control of the affected part of the brain. The same occurs from a hemorrhagic stroke.
When someone has a silent stroke, the interruption in blood flow occurs in part of the brain that doesn’t control any vital functions. Even though it doesn’t cause any obvious symptoms—most people who have had a silent stroke aren’t aware that it occurred, though the damage is revealed on an MRI or CT scan.
Memory can be affected by silent strokes, especially if several of them occur over time (which happens a lot). The damage from silent strokes can accumulate, which leads to more and more memory problems.
What can women do when faced with a stroke that has no symptoms, and that are only found on an MRI or CT scan? “I think that it should make people aware that it’s imperative to manage risk factors,” says Karen Furie, associate professor at Harvard Medical School and director of the Massachusetts General Hospital Stroke Service. This means:
–not smoking
–controlling blood pressure and diabetes
–aiming for a healthy weight
–keeping cholesterol levels in check
–managing atrial fibrillation
When someone experiences memory loss it should not be dismissed it as a normal part of aging. The doctor should be consulted for testing to make sure their isn’t a silent stroke.
The public should also be aware of the solutions available when a major stroke occurs and when physical therapy is needed to rehabilitate affected limbs.
The newly developed HANDTUTOR and its sister devices (ARMTUTOR, LEGTUTOR, 3DTUTOR) have become a key system in neuromuscular rehabilitation for stroke victims and those recovering from brain and spinal injuries,Parkinson’s, MS, CP and other limb movement limitations. These physical therapy products implement an impairment based program with augmented motion feedback that encourages motor learning through intensive active exercises and movement practice. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR consist of wearable glove and braces that detect limb movement showing the patient how much active or assisted active movement they are actually doing. The software uses special rehabilitation games to set a new target for this movement in terms of the patient’s ability to move their limb. The devices then measure the limb movement and give feedback to the patient. In this way the patient understands which effort is more successful. The TUTOR system provides exercises that are challenging and motivating and allow for repetitive and intensive exercise practice. The TUTOR system is now part of the rehabilitation program of leading U.S. German, Italian, French, UK and other foreign hospitals. IThey are also available throughthe use of telerehabilitation.See WWW.MEDITOUCH.CO.IL for more information.
Thursday, 14 June 2012
When Skilled Nursing Care is Needed
Once a patient completes his stay in an acute hospital the next step is to decide if he can go home and receive the care he needs there or whether he is better off in a nursing home or rehabilitation facility. Sometimes recovery at home will be slower than if the patient goes to a professional follow up care facility.
The choice to return home or not may be based on the following criteria:
Can the patient receive the care needed at home by family, friends or other caregivers?
Can the patient maneuver from and to a bed and chair without much help?
Can the patient walk around enough to be able to get to the bathroom and back?
If necessary, can the patient go up and down the stairs independently?
Can he prepare food and feed himself?
In short, is the patient able to take care of himself sufficiently or is more assistance needed?
Other factors which come into play are the illnesses that exist and whether the patient can take his own medicine correctly, care for any wounds and how mobile he is. Depending on the original reason for the hospitalization a nursing facility can assist with post acute care for knee, hip or shoulder surgery; stroke or brain injury care and other professionally needed assistance for the hospitalization.
A good skilled nursing facility is stocked with all kinds of equipment to facilitate the rehabilitation of its patients. the patients and their caregivers or family should visit several that are located in the area desired ahead of time to see if they are clean and cared for, have any undesirable odors, seem to be staffed adequately and in general have a good reputation.
The care that is provided by a skilled nursing facility includes: periodic visits by the patient’s physician, trained health professionals that will administer rehabilitation, wound care, medication administration, social workers to see that everything necessary is being done and to prepare for aftercare, therapists to teach ADLs, speech and language specialists, if necessary and any other professionals needed to pave the way for a return home.
If physical therapy is needed then the best equipment should be available. This may include the TUTOR system for patients that suffered a stroke or other limb debilitating injury or disease. The TUTORs are physical therapy products that are used as solutions for patients who have had a stroke, Parkinson’s, CP, MS, brain/spinal cord injuries, radial and Ulnar nerve injuries, development disorders, Brachial Plexus injuries or other upper or lower limb surgeries that cause paresis of a limb.
The TUTOR system which consists of the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are comfortable ergonomic gloves or braces that implement an impairment based rehabilitation program with augmented feedback and encourage motor learning. This is accomplished through exclusive software that allows the therapist to evaluate, objectively quantify and record the patient’s impairments. Currently in use in leading U.S. and European hospitals and rehabilitation clinics the TUTOR system is also available in patient’s homes through the use of telerehabilitation. The TUTORs are available for use by children as well as adults and are fully certified by the FD and CE. See WWW.MEDITOUCH.CO.IL for more information.

Wednesday, 13 June 2012
Knee Surgery and Its Prevention
Much has been written about knee surgery and the innovations made to replace them. It’s the largest joint in the body. The knee helps you stay active, flexible and is an essential role in facilitating movement. And in spite of the fact that any problem/injury affecting the knee would have the power to immobilize it, it is one the most overlooked aspects of health care.
No one can deny that we often worry about our knees only after a crippling pain begins. However at this point, the damage has already been done and replacement surgery is sometimes the only option. However, knee problems don’t happen suddenly. It’s a slow process that occurs within the first 40 years of life and because of bad lifestyle choices and genetics.
The knee is protected by cartilage — a soft, flexible, connective tissue that is softer than bone but harder than muscle. It forms a cover and links the two major bones of the leg. Damage to this cartilage can be painful and irreversible and therefore surgery becomes a necessity.
Knee cartilage health can be affected by many factors, according to Dr. J.V.Srinivas , senior orthopaedic surgeon, Fortis Hospital, Bangalore, India. In osteoarthritis, the … cartilage is completely worn out, until one bone rubs against another. It’s a result of a process of degeneration, due either to a very active lifestyle or a severe lack of calcium. Women are particularly at risk. Women in our culture get married early and have on average two or three children in their twenties. These women lack calcium and by the time they reach 40, they are affected by osteoporosis, a bone brittling and calcium deficient disease that can put them at risk for fractures and degeneration of the knee cartilage. Inflammatory arthritis (which is extreme swelling or pain in addition to the degeneration of cartilage) can cause severe damage as well but this occurs as a result of genetic factors and diseases and therefore can hardly be avoided.
In most cases, damage to the cartilage is due to the process of aging. But there are ways one can protect himself against the pain and prevent more damage. According to Dr. Srinivas it’s important to maintain good body weight. Overweight or obese people will only put more pressure on their knees.
Regular exercise will help joints stay mobile and flexible. A timely diagnosis and the control of diabetes and hypothyroidism are important too, because if not kept in check it could affect healthy cartilage.”
Starting to take care of knee health should occur at childhood. Dr. Srinivas says that the more active one is the more nutrition is being fed to the knee cartilage. A lot of children lead sedentary lives and stay glued to computer screens and TV. Because bone health peaks between the ages of 20-40, one should maintain participation in sports and be active as much as possible during those years. After the age of forty, men and women lose at least 3% of their bone calcium per year. It is impossible during those years to build calcium reserves and taking calcium pills won’t work. Most Americans and Europeans engage in sports during these crucial years, so for this age population, knee problems usually occur in the eighties. For the average citizen knee problems crop up as early as the forties, which can severely threaten our mobility and add greater discomfort to old age.
Here are some precautions: 1-Don’t worsen knee pain by climbing stairs or sitting cross-legged on the floor. 2-Try to sit on chairs or a raised surface until the pain recedes. 3-Avoid walking on hard gravelly surfaces or performing strenuous exercises while in pain. 4-Rest is best . 5- Switch to low impact activities like swimming and walking.
People that have advanced osteoarthritis can avail themselves of knee replacement surgery. This is fast becoming a common procedure in many countries.
The surgery can be expensive depending on the hospital and post-surgical care. The surgery involves partially or completely replacing the knee. Recovery can take from 3-6 weeks, after which one can usually return to normal life. The pain should have completely receded and the knee should be as good as new. Following surgery, doctors usually advise the patient to have an active lifestyle to help further weight loss and to prevent fresh damage to the knee joints. Caring for knees is a lifelong process. After all, it’s because of this joint that we have the ease and freedom of mobility.
While recuperating from knee surgery physical rehabilitation will occur. One of the most cost effective and efficient physical therapy solutions is the LEGTUTOR.
The LEGTUTOR is an ergonomic wearable leg brace with dedicated rehabilitation software. The LEGTUTOR rehabilitation concept is based on performing controlled exercise rehabilitation practice at a patient customized level with real time accurate feedback on the patient’s performance. This means that the LEGTUTOR system allows the physical therapist to prescribe a leg rehabilitation program customized to the patient’s knee and hip movement ability at their stage of rehabilitation. The LEGTUTOR uses biofeedback to keep the patient motivated to do the exercise practice in the form of challenging games. The TUTORS, (HANDTUTOR, LEGTUTOR,ARMTUTOR, 3DTUTOR) are suitable for a wide variety of other neurological and orthopedic injuries and diseases as well as post trauma and orthopedic surgery.
The TUTOR system is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. It is designed for children and adults and can be used at home supported by telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.
Strengthening Leg and Hip Muscles and Other Exercises
Harvard Medical School has released some guidelines for effective treatment for several knee and hip problems. Indicating that it is more than just a good health habit, exercise can be effective for many lower extremity problems. Strengthening the muscles around damaged hips and knees can support those joints by taking over some of its responsibilities. If your surrounding muscles (gluts, hamstrings, quads or abdominal) are strong they will be able to support body weight. Strong quads can take over shock absorbing roles.
Proper balance of the muscles can hold the joint in the best and most functional way to prevent pain.Usually the first muscles to lose strength are the large muscles so it would be important to maintain focus on those. Working in pairs muscles either contract or relax. If there is imbalance it can cause injury and other joint problems.
For example, if your hamstrings are tight, your quadriceps can’t contract fully and may weaken, so one should exercise the quadriceps and hamstrings (the opposing muscles) equally. Another suggestion is to do flexibility exercises ( stretching and relaxing specific muscles) to improve joint function.
Physical therapists have emphasized the distinction between open-chain and closed-chain exercises. The ”chain” meaning a series of body parts, such as a hip, knee, ankle, and foot.
In an open-chain exercise, the body is stationary while the limb moves. In closed-chain exercise, the limb is stationary while the body moves. For example, a squat is a closed-chain exercise. A seated leg extension is an open-chain maneuver.
After ACL injury open-chain exercises may be more effective for increasing quadriceps strength .
Physical therapists are mostly incorporating closed-chain exercises into rehabilitation programs and recommending them for people that have painful joints because these exercises involve more muscles and joints and thus help to create stability around a joint.
Using a physical therapist can be very helpful and because he will individualize your treatment program to restore or maintain your physical functioning for arthritis and other joint problems.
The therapist evaluates your functional ability, pain, strength, and endurance. A session with the physical therapist may involve pain-relieving treatments using ice, heat and massage. The physical therapist also supervises you in your exercises and explains exercises that can be done at home. Sometimes there may be a pool and other exercise equipment to use.
Gait training is a major component of physical therapy. Having knee and hip problems can disturb normal walking by causing pain, restricting joint movement, or weakening muscles. Standing, walking, or running may also cause joint problems if weakness in key muscles, poor coaching advice, or bad habits throw off the correct gait.
It could take years of walking with an abnormal gait before joint injury occurs and improper running can lead to pain and injury more rapidly because it involves greater force with each stride.
One of the duties of a physical therapist is to analyze your gait and help you learn to walk more normally. Initially, the proper gait may feel odd, but in time, it becomes comfortable. Sometimes a change in shoes or specific exercises to strengthen muscles may be necessary.
After knee or hip replacement there is a tendency to lean towards the operated leg therefore it is important to get retrained on how to stand straight and use both legs evenly. Gait retraining may be accomplished best by using the buoyancy of a swimming pool to learn how to stand straight and reduce the fear of falling.
When the knee or hip is replaced a new state of the art physical therapy solution is the TUTOR system. Specifically the LEGTUTOR is used to allow the patient to accomplish a series of intensive and challenging exercises. The LEGTUTOR consists of a safe and comfortable leg brace with position and speed sensors that precisely record three dimensional hip and knee movements. The LEGTUTOR has a range of motion limiter that can limit the dynamic range of knee extension and flexion. Rehabilitation games allow the patient to exercise range of motion, speed and accuracy of movement. The LEGTUTOR facilitates evaluation and treatment of the lower extremity including isolated and combined hip and knee movements. The LEGTUTOR and its sister physical therapy products (HANDTUTOR, ARMTUTOR, 3DTUTOR) are already in use in leading U.S. and Eurpopeean hospitals and clinics. They are suitable for adults and children and also through telerehabilitation. They are FDA and CE certified. See WWW.MEDITOUCH.CO.IL for more information.

Monday, 11 June 2012
The Wolf Test and Stroke Rehabilitation
The Wolf Motor Function Test for Stroke Patients asseses and monitors upper extremity function in stroke patients and others who have injuries that limit normal motor function. In a report issued by Emory University on June 9, 2012 there is a description of the benefits of this test.
It Includes a protocol and physical template that can be standardized and used regularly by a physical therapist or physician to evaluate the patient‘s improvement.
It is more sensitive to individual changes in motor abilities than many other tests.
It is easier to administer and requires less equipment than similar tests.
In the US there are approximately 750,000 stroke victims each year. Of those 400,000 have physical and/or neurological disabilities. In addition over 80% of strokes affect upper limb movement, which results in a decreased quality of life for patients and necessitates the need for a caregiver. There are other motor function tests but they are more difficult to administer.
Sometimes a limb is not paralyzed, but the difficulty introduced by an impairment can result in “non-use” of the affected arm. This ”limb choice” is not represented well in neuro-rehabilitation research and treatment. INTENSIVE MOTOR TRAINING OF THE AFFECTED LIMB CAN GREATLY IMPROVE PERFORMANCE IN STROKE PATIENTS.
The Wolf Motor Function Test provides a standardized protocol for assessing upper extremity function and tracking improvements in stroke patients and those who have suffered other injuries that limit normal motor function of the arms and hands. The test measures the patient’s performance during general movements of the upper extremities, including reaching, lifting, gripping and fine motor control. It also allows for comparison of the mobility of the affected and unaffected upper limbs. The test consists of a scripted protocol that describes in detail the conditions under which the test should be administered i.e. the sitting position, camera placement, and a description of items to be used during the test. It also includes a physical template and instructions as to how to use the template during the test. Guidelines are specified in the protocol which enable standardization and finely tuned monitoring of motor function of the upper extremities. The test is also able to detect smaller degrees of change in performance (compared to other tests) and may be prescribed by a physical therapist or physician to be performed on a regular basis by stroke patients to aid in their recovery.
Leading the way in upper extremity physical therapy solutions is the ARMTUTOR and the HANDTUTOR.
The ARMTUTOR and HANDTUTOR systems have been developed to allow for functional rehabilitation of the upper extremity including the shoulder, elbow and wrist. The system consists of an ergonomic wearable glove and arm brace together with dedicated rehabilitation software. The ARMTUTOR™ and HANDTUTOR systems allow the physical and occupational therapist to report on and evaluate the patient’s functional rehabilitation progress. This allows the OT and PT to prescribe the correct customized and motivating intensive exercise practice to the manual rehabilitation therapy. Intensive repetition of movement is achieved through challenging games set to the patient’s ability. The system provides detailed exercise performance instructions and precise feedback of the patient’s efforts. Controlled exercise of multijoints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks. Telerehabilitation allows the recovering patient to continue his physical therapy at home. The system, which also includes the LEGTUTOR and 3DTUTOR, is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. See WWW.MEDITOUCH.CO.IL for more information.
Sunday, 10 June 2012
What Exactly is a Brain Concussion and What Treatment is Helpful?
There are so many occurrences of brain concussion especially amongst young athletes that it behooves everyone, especially those involved in sports, to be aware of what happens, how to prevent it and what the treatments are for it.
What is concussion and what causes concussion?
What is referred to as ”mild traumatic brain injury” or concussion, can be defined as a temporary loss of brain function due to a trauma to the head. With concussion, function may be interrupted but there is no structural damage to the brain.
The brain ”floats” in cerebrospinal fluid and is encased in the skull. These protections allow it to withstand many minor injuries that occur daily. However, if there is sufficient force that causes the brain to bounce against the bones of the skull, then there is potential for injury. It is the movement of the brain against the inside of the skull that can cause the brain to be irritated and thereby interrupt its function. This movement can come from a direct blow to the head or face, and also from other body trauma that can cause the head to shake. Temporary loss of consciousness due to the injury probably means that a concussion has taken place however there are concussions that occur without the patient being knocked out. To be sure there are studies of football players where the majority aren’t even aware that they had sustained a head injury.
Types of concussion?
Traditionally, the severity of concussion was based on the loss of consciousness and its duration together with the presence of amnesia. It was presumed that there was a correlation between those two events and the amount of potential brain damage.
According to The International Conference of Concussion in Sports concussion be divided into two groups: simple and complex.
Simple concussion: In a simple concussion, the symptoms gradually resolve, and the patient returns to normal function in seven to 10 days.
Complex concussion: In complex concussions, symptoms remain and thought processes are affected. Patients who have repeated concussions would fall into the complex category.
The Mayo Clinic recommends the following preventions.
1-Sports players should wear appropriate protective gear during games and other recreational activities. The equipment should fit well, be maintained and worn correctly. Players should follow rules and play responsibly and in a sportsmanlike way. Cyclists of any kind of vehicle should wear protective headgear.
2-Buckle your car seat belt. The belt can prevent an injury to the head in case of an accident.
3-Make your home safe. Since falls around the home are the leading cause of head injury for infants, toddlers and older adults it’s important to keep the home well lit and floors free of objects — meaning anything that might cause someone to trip and fall..
4-Protect your children. To help lower the risk of head injuries to children, it’s a good idea to place padding around countertops and edges of tables. If there are very young children in the house, block off stairways and install window guards. Don’t let children play sports that are not at their age level.
5-Use caution in and around swimming areas. Don’t dive into a pool that is less than 9 feet (3 meters) deep. Follow posted safety rules at water parks and public pools.
6-Wear sensible shoes. Wear shoes that are easy to walk in. Don’t wear high heels, sandals with thin straps, or shoes that are either too slippery or too sticky.
Concussion Treatment
When there is bleeding under the scalp, but outside the skull, it creates a “goose egg” or large bruise, called a hematoma, at the site of the head injury. Generally this hematoma will go away on its own with time.
The use of ice immediately after the trauma may help decrease its size however do not apply ice directly to the skin. Rather use a washcloth as a barrier and wrap the ice in it. One can also use a bag of frozen vegetables wrapped in cloth, as this conforms nicely to the shape of the head.
Ice should be applied for 20-30 minutes at a time and repeated every two to four hours. After 48 hours there is little benefit to icing.
Resting is important to allow the brain to heal.
The patient should be seen by a professional health expert as soon as possible.
According to the American Academy of Neurology any athlete suspected of having a concussion should be removed from play until evaluation by a physician. If a concussion is suspected , the Centers for Disease Control recommends implementing a 3-step plan:
1-The player should immediately stop playing and not return until the doctor approves.
2-Do not try to judge the severity of the injury yourself but rather have a professional do it.
3-Inform the athlete’s family about the possible concussion and give them vital information about concussions.
If a second concussion occurs before the brain has recovered from the first one it can slow recovery or even increase the likelihood of having long-term problems. In some cases, repeat concussions can result in edema (brain swelling), brain damage, and even death.
If, unfortunately, brain damage occurs and it results in paresis of one or more limbs then after the acute stage it is important to use the best physical therapy solution available. One of the most cost effective and efficient physical therapy products available is the TUTOR system. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are products that are used to allow intensive exercise therapy to the brain injured patient.
The newly developed HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have become a key system in neuromuscular rehabilitation and physical therapy for interactive rehabilitation exercise. These innovative products implement an impairment based program with augmented feedback and encourage motor learning through intensive active exercises. These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. The training is customized by the occupational and physical therapists to ensure that the patient stays motivated to do intensive repetitive manual therapy and exercise practice. The TUTOR system is now part of the rehabilitation program of leading U.S. and foreign hospitals where they are used in rehabilitation clinics and in the patient’s home through the use of telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.
Subscribe to:
Posts (Atom)