Showing posts with label stroke. Show all posts
Showing posts with label stroke. Show all posts
Tuesday, 7 August 2012
New Formula Predicts Rehabilitation Outcome
The journal called ”Brain” featured an article on July 31, 2012 about a development that could revolutionize rehabilitation for stoke patients. University of Auckland researchers have shown how it may be possible to predict potential recovery in stroke patients for hand and arm function. Realistic goals for recovery may be set for patients and trial outcomes for new therapies may have also have better results through this approach.
According to Professor Winston Byblow one of every six people will have a stroke at some time during their life and until now comparisons were made as to outcome based on group similarity to others with the same symptoms. An individual patient’s rehabilitation plan can not be known. ”We have developed the first clinical algorithm to actually predict the individual patient’s potential for recovery based on information gathered before rehabilitation even begins.” said Byblow.
A test is administered to the hospitalized stroke patient within 3 days of the event. It is very quick and requires no special equipment. Dr Cathy Stinear, who authored the journal article, explains that in some cases additional testing may be required such as an MRI to determine whether the pathways in the particular side of the brain remain viable and to measure the integrity of neural pathways from the brain to the arm. When the algorithm is combined with the results of the tests a prediction can be made about patient recovery at 12 weeks which is when therapy would normally end.
The information gleaned from this new test can be used to customize rehabilitation for the patient before it even begins. It is the first study to predict an individual’s potential for motor function recovery using test results obtained from that patient in the first days after stroke, according to Neurologist Professor Alan Barber, a member of the research team and Head of the Auckland Hospital Stroke Service .
The research team is now in a three year trial period of the algorithm method to show if the outcomes really benefit the patient and increases the efficiency of hospital rehabilitation services.
Once that prediction is made and actual rehabilitation commences the physical therapy product of choice may well be the HANDTUTOR and ARMTUTOR.
The HANDTUTOR and ARMTUTOR™ have been developed to allow for functional rehabilitation of the upper extremity including the shoulder,arm, elbow and wrist. The system, recommended for use for a variety of injuries and diseases including stroke, Parkinson’s, CP, MS and other upper and lower limb disabilities
, consists of an ergonomic wearable glove and arm brace together with dedicated rehabilitation software. The TUTOR systems (including the LEGTUTOR and 3DTUTOR) allow the physical and occupational therapist to report on and evaluate the patient’s functional rehabilitation progress. This allows them to prescribe the correct customized and motivating intensive exercise practice to the manual rehabilitation therapy. Intensive repetition of movement is achieved through challenging games set to the patient’s ability. The system provides detailed exercise performance instructions and precise feedback on the patient’s efforts. Controlled exercise of multijoints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks. Telerehabilitation allows the recovering patient to continue his physical therapy at home. The system is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. See WWW.MEDITOUCH.CO.IL for more information.

Thursday, 26 July 2012
Meaningful Task-Specific Training (MTST) Works With Stroke Rehabilitation
K.N. Arya etal of the Department of Neurology, CSM Medical University, Lucknow, India in a study published in Top Stroke Rehabilitation in the May/June 2012 edition discuss the following study they conducted.
One of the functional challenges in post stroke patients is the upper extremity motor deficit. The objective of this study was to evaluate the results of the ”meaningful task-specific training” (MTST) on upper extremity motor recovery during the subacute phase after a patient suffers a stroke.
The study was conducted as a randomized, controlled and double-blinded trial in the neurology department of a university hospital and occupational therapy unit of a rehabilitation facility. A sample of 103 people post stroke, was randomized into 2 groups (the MTST group had 51 participants and the standard training group had 52). Ninety-five of the participants completed the 8-week follow-up program. Participants were assigned to receive either the MTST or dose-matched standard training program based on the Brunnstrom stage and Bobath neurodevelopmental technique, 4 to 5 days a week for 4 weeks.
The results showed a positive improvement in the scores of the MTST group at post and follow-up assessments in comparison to the control group. In addition, statistically significant differences were observed in changes between the groups at post and follow-up assessment for FMA, ARAT, GWMFT, and MAL.
The conclusion drawn was that the MTST group produced statistically significant results as well as clinically relevant improvements in the upper extremity motor recovery of the patients who had had a subacute stroke.
When providing physical therapy solutions for upper extremity movement disorders the ARMTUTOR is one of the leading and most cost effective products available.
The ARMTUTOR™ has been developed to allow for functional rehabilitation of the upper extremity including the shoulder, elbow and wrist. The system consists of an ergonomic arm brace together with dedicated rehabilitation software. The ARMTUTOR™ system and its sister devices (HANDTUTOR, LEGTUTOR, 3DTUTOR) allows the physical and occupational therapist to report on and evaluate the patient’s functional rehabilitation progress and then to prescribe the correct customized and motivating intensive exercise practice to the manual rehabilitation therapy. Intensive repetition of movement is achieved through challenging games set to the patient’s ability. The system provides detailed exercise performance instructions and precise feedback on the patient’s efforts. Controlled exercise of multijoints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks. Telerehabilitation allows the recovering patient to continue his physical therapy at home. The system is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. See WWW.MEDITOUCH.CO.IL for more information.

Monday, 23 July 2012
Improving Brain Function After Stroke
Dr. Robert Rennaker and Dr. Michael Kilgard of the University of Texas, Dallas recently proved how nerve stimulation when paired with specific experiences, like movements or sounds, is able to reorganize the brain and even improve its function.
What they discovered could lead to new treatments for stroke, autism, tinnitus, and other disorders.
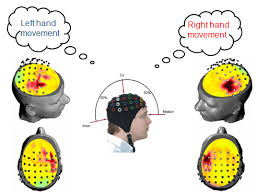
The researchers looked at whether by repeatedly pairing vagus nerve stimulation with a specific movement it would change neural activity in laboratory rats’ primary motor cortex. They paired the vagus nerve stimulation with movements of the front limbs in two groups of rats.
After a period of five days of this stimulation and movement pairing, the researchers examined the brain activity of the rats. Those who received the training together with the stimulation displayed large changes in the organization of the brain’s control system. Those animals receiving identical motor training without stimulation pairing didn’t exhibit any brain changes, known as plasticity.
Patients suffering from strokes or other brain trauma often have rehabilitation that includes repeated movement of the affected limb in order to regain motor skills. It is surmised that repeated use of the affected limb will cause reorganization of the brain which is essential to recovery.
Dr. Rennaker stated that there was a suggestion from the research that pairing vagus nerve stimulation with standard therapy could result in a more rapid and extensive brain reorganization. This would offer the potential for speeding recovery following a stroke.
He further stated “Our studies in sensory and motor cortex suggest that the technique has the potential to enhance treatments for neurological conditions ranging from chronic pain to motor disorders. Future studies will investigate its effectiveness in treating cognitive impairments”.
Vagus nerve stimulation has an excellent safety record in human patients that suffer from epilepsy. Therefore the technique researched provides a new method to treat brain conditions such as dyslexia and schizophrenia.
Future human patients may have access to more efficient therapies that are minimally invasive and avoid long-term use of drugs if the studies are confirmed.
To provide repeated movement of a stroke affected limb the TUTOR system has been in the forefront of physical therapy products. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been developed to provide intensive and active movement of disabled legs, hands, wrists, elbows and other upper and lower limbs. The ergonomic gloves and braces that make up the TUTOR system are connected to dedicated software that allows the therapist to fully customize the exercises to the patient’s movement ability. In addition the therapist can objectively and quantitatively evaluate and report on the treatment progress. The TUTOR rehabilitation system optimizes the patient’s motor, sensory and cognitive performance and allows him to better perform everyday functional tasks to improve their quality of life.
The TUTOR system is currently in use in leading U.S. and European hospital and clinics. They are fully certified by the FDA and CE and can be used at the patient’s home via telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Sunday, 22 July 2012
Can Prayer Help Prevent Stroke?
Do you want to prevent having a stroke? One of the most important methods is to eliminate any risky practices you may have. Of course there are certain things we can’t change such as: genes, age and gender but we can change diet and physical activity.
Adopting a diet which is low in salt and fat but high in fiber is a beginning. Vitamin B rich foods such as spinach, broccoli, carrots, salmon, herring, chicken, walnuts, almonds, sunflower seeds and whole wheat would be helpful. It is known that Vitamin B foods lower homocysteine levels and too much of this amino acid in the blood increases the risk for stroke. There are other foods that lower the risk of stroke and they include cinnamon, garlic, olive oil, onion, dark chocolates, green tea, oatmeal and strawberries.
People that have diabetes should take necessary steps to prevent stroke as well. Diabetics are at risk and therefore should manage their diabetes by eating healthy and monitoring their blood pressure.
Exercise is is a crucial element in stroke prevention as obesity is a stroke risk. Exercise will help take off pounds and maintain healthy weight. Cholesterol levels should be checked regularly.
The state of one’s mental health can also increase stroke risk. Stress can be very damaging, if left unmanaged. It raises blood pressure, which makes the heart pump harder. One of the ways to reduce stress is with physical activity such as exercise or deep breathing. Reading and prayer or meditation can also relieve stress.
Preventing high blood pressure is crucial to stroke prevention. That can be done by avoiding, or at least reducing, the consumption of high-fat foods such as: butter, red meat, eggs, shortening, certain cheeses and dairy products. Reducing the amount of salt is advisable. Sugar, caffeine and alcohol can raise blood pressure, which is a risk factor of stroke.
Here are some common symptoms of stroke which, if experienced, should be brought to the attention of medical experts immediately. Sudden weakness or numbness in the face or limbs; slurred speech or drooling; numbness on one side of the body; problems with balance or walking; dizziness; confusion; or a severe headache.
Unfortunately, even with the best prevention, stroke can still occur and one of the after effects can be the paralysis of a limb. When that occurs and after the patient is stabilized the emphasis will be to rehabilitate the leg or arm that is affected. Fortunately, today there are some very good physical therapy solutions such as the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR.
The TUTOR system has become key in neuromuscular rehabilitation for stroke victims and those recovering from brain and spinal injuries, Parkinson’s, MS, CP and other limb movement limitations. These innovative devices implement an impairment based program with augmented motion feedback that encourages motor learning through intensive active exercises and movement practice. They consist of a wearable glove or braces that detect limb movement showing the patient how much active or assisted active movement he is actually doing. The rehabilitation software uses special games to set a new target for this movement in terms of the patient’s ability to move their limb. The devices then measure the limb movement and give feedback to the patient in trying to gain this new movement objective. Consequently the patient understands which effort is more successful in getting him to move their affected limb again. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are now part of the rehabilitation program of leading U.S. German, Italian, French, UK and other foreign hospitals. They are adaptable for children as well as adults and are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.

Monday, 16 July 2012
How Much Salt to Add to Your Food
As published on Wednesday, April 25, 2012 in the journal STROKE, Dr. Francesco P. Cappuccio, of the University of Warwick in the UK stated that older adults with salty diets may have an increased risk of suffering a stroke.
The results were in a study of 2,700 older, mostly minority adults. They got well above the recommended sodium intake and were nearly three times as likely to suffer a stroke over 10 years as people who met guidelines recommended by the American Heart Association (AHA).
As people’s sodium intake goes up, their blood pressure will likely increase as well.
What is not as clear, though, is whether a salty diet may mean higher risks of heart attack and stroke later on.
Unlike blood pressure, which can change quickly, stroke and heart disease are more long-range complications. So a study of the relationship between people’s sodium intake and their risk of heart problems and stroke is more difficult.
At this time, the AHA suggests that people not consume more than 1,500 milligrams a day. The World Health Organization advises a limit of 2,000 milligrams.
The people in this study — mainly black and Hispanic New Yorkers — consumed 3,031 milligrams of sodium per day.
The findings are based on 2,657 adults who were interviewed about their health and lifestyle and then completed dietary questionnaires. They were 69 years old, on average, when the study began.
During the next 10 years, there were 235 strokes in the group. Those that downed 4,000 or more milligrams of sodium each day were almost three times more likely to suffer a stroke as those who kept their daily sodium below 1,500 milligrams.
Among the 558 people consumed more than 4,000 milligrams per day, there were 66 strokes.
That compared with 24 strokes among the 320 people who kept within the AHA guideline.
Hannah Gardener, a researcher at the University of Miami School of Medicine who led the study said “We can’t definitively draw conclusions about cause-and-effect .
There can be a number of other factors to take into consideration in addition to salt intake. As an example
smoking habits, exercise levels, education and health conditions like diabetes and high blood pressure need to be taken in to consideration.
Although few Americans adhere to the AHA guidelines they should be followed according to Gardener.
Interestingly, it’s estimated that the typical U.S. man takes in 4,000 milligrams of sodium a day, while women typically ingest 2,800 milligrams.
Salt is pervasive in the food supply — from canned soups and sauces, to breads and cereals, to processed meats — and it can be challenging to cut down. Americans receive almost 80 percent of their sodium from prepared foods on supermarket shelves and in restaurants, rather than at home.
Gardener further states that it is important to read product labels to know beforehand how much sodium there is in the product.
Eating fruits, vegetables and whole grains, as much as possible will also alleviate the problem.
The researchers suggest that responsibility should also rest on government regulations and the food industry.
In England, the government has begun to regulate the processed food industry. New York City has instituted the National Salt Reduction Initiative. This move tries to coordinate local and state governments and health groups to work with the food industry to cut sodium in packaged foods and restaurants.
Heinz, Kraft Foods and Starbucks, have already signed on to meet salt targets.
Unfortunately, at this time and age people still take in too much sodium so strokes will still occur. When they do and the initial medical treatment is completed it behooves doctors and other medical staff and facilities to supply the best physical therapy solutions available to treat any paralysis that may exist as a result of the stroke. Such physical therapy products are the TUTOR system.
Rehabilitation using the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR is instituted in the USA at major in-patient and out-patient clinics as well as at private physical therapy clinics. Many patients including stroke victims can also avail themselves of the TUTOR system through the use of tele rehabilitation when they are at home or in a location far from a qualified rehabilitation center. The TUTOR products have been developed to allow for functional rehabilitation of the whole body including the upper and lower extremity. The system consists of ergonomic wearable devices and dedicated rehabilitation software that provide patient instructions and feedback to encourage intensive controlled exercise practice. The TUTOR system exercises multijoints within the normal movement pattern which prevents the development of undesired and compensatory joint movement. It therefore ensures better performance of functional tasks. This is important in stroke, brain, spinal cord (SCI) and Cerebral Palsy rehabilitation in addition to other neurological and orthopedic injury and disease. Additional features of the TUTOR system include quantitative evaluation and objective follow up that is important in the physiotherapists treatment of the stroke patient. The TUTORS are FDA and CE certified and are available for children as well as adults. See WWW.MEDITOUCH.CO.IL for more imformation.
Monday, 9 July 2012
Action Observation Treatment (AOB) as a Means of Physical Rehabilitation
AOB may be defined as when the observation of actions performed by others activate in an observer the same neural structures as when he/she actually performs the same actions.
There is evidence that the observation of actions activates the same cortical motor areas that are involved in the actual performance of the observed actions. The neural substrate for this is the mirror neuron system. We capture this neuronal system and then re-enact the stored motor representations as a means for rehabilitating motor control. This may be called motor imagery.
In a study employing AOB eight stroke patients with moderate, chronic motor deficit of the upper limb participated. A significant improvement of motor functions during a 4-week treatment, as compared to the stable pre-treatment baseline, and compared with a control group was found. The improvement lasted for 8 weeks after the end of the intervention.
Physical rehabilitation, for a large part may be seen as a learning process where old skills have to be re-acquired and new ones have to be learned on the basis of practice. Active exercising creates a flow of sensory information. It is known that motor recovery and motor learning have many aspects in common. Both are largely based on response-produced sensory information. Numerous studies have indicated that motor imagery may result in the same plastic changes in the motor system as actual physical practice. Motor imagery is the mental execution of a movement without any overt movement or without any peripheral (muscle) activation. It has been shown that motor imagery leads to the activation of the same brain areas as actual movement. Therefore motor imagery may play an important role in neurological rehabilitation. Furthermore, the observation of a movement may play a similar role in learning movement. The use of motor imagery in neurological rehabilitation may have a value even if it’s on theoretical grounds and on the basis of the results of studies with healthy subjects.
For actual physical therapy solutions for stroke patient rehabilitation the TUTOR system is one of the most effective products available. The TUTOR system, consisting of the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR, are ergonomic gloves and braces with speed and position sensors that are placed on affected parts of the body. Specialized powerful software is used to allow the patient to exercise his affected limb. The information is then recorded and evaluated by the physical therapist who then designs a customized exercise plan for that patient. The TUTORs are currently in use in leading U.S. and European hospitals and clinics and are fully certified by the FDA and CE. The patient can avail himself of the TUTOR system at home through the use of telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.
Tuesday, 14 February 2012
Tutor system - LegTutor effective tool with intensive robotic and manual gait training in sub-acute stroke

In the February edition of Journal of NeuroEngineering and Rehabilitation Dr. Conesa and his group from Functional Rehabilitation Department and the Brain Injury Unit, Neurorehabilitation Hospital Institut Guttmann Barcelona, Spain and the Harvard Medical School, Boston, MA, USA report that 8 weeks of intensive physical rehabilitation including robotic and manual gait training was well tolerated by early stroke patients. The group saw significant gains in function with outcome measures including improved walking speed and balance scales. In particular, robotic training on the mid-level gait dysfunction group showed the best improvement. The gait training was split up into robotic gait training from 0-4 weeks and manual gait training weeks 4-8.
The LegTutor is a Leg brace that measures hip and knee movement. it is used to customize isolated and intensive manual gait exercsie practice and give the patients augmented feedback on their performance. The 3DTutor can be used to give intensive ankle exercise practice and assist in treating drop foot.
Friday, 18 November 2011
LegTutor Used in TeleRehabilitation for Knee Replacement Therapy

SHARON WORCESTER, Family Practice News Digital Network on November 17, 2011 reports from Chicago that
patients who undergo total knee replacement surgery recover just as well with postoperative, group-based, outpatient physiotherapy or a monitored, home-based physiotherapy program as with a one-on-one, outpatient center–based program, according to findings from a randomized study involving 249 patients.
With the exception of patient satisfaction with physiotherapy – which was significantly greater for the 85 patients who were randomized to one-on-one therapy and the 84 who were randomized to group-based therapy than it was for the 80 patients who received home-based therapy (mean satisfaction rates, 90%, 84%, and 73%, respectively) – no significant differences were seen in any other outcome measures during the first postsurgical year, Victoria W.M. Ko of the University of New South Wales, Sydney, and her colleagues reported in a poster at the annual meeting of the American College of Rheumatology.
For example, WOMAC (Western Ontario and McMaster Universities) Osteoarthritis Index function scores at postoperative week 10 (the primary outcome measure) were similar at a mean of 44.0, 39.32, and 35.0 in the one-on-one patients, the group-based therapy patients, and the home-based therapy patients, respectively. There also were no differences among groups in recovery of mobility as measured by a 6-minute walk distance and a timed stair test, or inHRQOL (Health-Related Quality of Life) score, knee range of motion, or patient-related overall recovery at 52 weeks, the investigators found.
Furthermore, the home-based program patients were no more likely than those in the other groups to be readmitted to the hospital or to experience any other complications.
Patient in the single-blind study were consecutive adults (mean age, 67 years) who were awaiting total knee replacement, were enrolled 2 weeks prior to surgery, and were randomized 2 weeks after surgery. During the 6-week therapy period, those who were randomized to receive one-on-one therapy or group-based therapy received 12 physiotherapy sessions, and those in the home-based program were prescribed home exercises supplemented with two sessions of one-on-one therapy and a telephone follow-up. All patients were assessed preoperatively and at postoperative weeks 2, 10, 26, and 52.
The findings are important because of the increasing volume of total knee replacement surgeries performed annually, and because home-based therapy provides a safe and more resource-efficient alternative to center-based physiotherapy, the investigators concluded. They added that this approach “will also circumvent access issues frequently associated with center-based care.
The LegTutor is being included extensively in home based physical therapy following knee replacement surgery through the use of telerehabilitation.
The LegTutor™ system has been developed to allow for functional rehabilitation of the lower extremity. The system consists of an ergonomic wearable leg brace and dedicated rehabilitation software. The LegTutor™ system, which includes the HandTutor, ArmTutor and 3DTutor, allows for a range of biomechanical evaluation including speed, passive and active range of motion and motion analysis of the lower extremity. Quantitative biomechanical data allow for objective evaluation and rehabilitation treatment follow up. The LegTutor™ rehabilitation concept is based on performing controlled exercise rehabilitation practice at a patient customized level with real time accurate feedback on the patient’s performance. The exercises are designed in the form of challenging games that are suitable for a wide variety of neurological and orthopedic injury and disease.
The games challenge the patient to perform the exercise task to their best ability and to continue exercise practice.
In addition the LegTutor™ allows for isolated and a combination of knee and three directional hip treatment. The Tutor system provides detailed exercise performance instructions and precise feedback on the patients exercise performance. Controlled exercise of multi joints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks.
The LegTutor™ system is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. See www.HandTutor.com for more information.
Tutor System Significant Factor in Spinal Cord Injury Rehabilitation

RICK HANSEN submits this story in Friday’s Globe and Mail Published Friday, Nov. 18, 2011 about Tracy Dort-Kyne, an Ontario mother of three who suffered a spinal cord injury after a cycling accident in September. I was fortunate to meet Tracy this month at Lyndhurst Hospital, where we spoke about her current situation and her future. I was touched by Tracy’s story – and impressed by her passion and conviction for a future where she’ll continue to be a participating member of society.
Medicare’s no match for catastrophic injury It requires specialized treatment and long-term care, amounting to billions of dollars annually in Canada. As Tracy’s story illustrates, once surgery and rehabilitation are complete, the challenges faced can be relentless – from painful secondary health complications to multiple barriers to reintegration. Further, as our population ages, tens of thousands of additional spinal cord injuries will occur from falls and illnesses, putting additional pressure on the health-care system’s ability to deliver high-quality, cost-effective care.
Great progress has been made in recent years, with current programs and initiatives that further aim to reduce the impact of spinal cord injuries on the health-care system, as well as on individuals and families. In the 25 years since I wheeled around the world, significant research developments have been made that reduce hospital stays for those with spinal cord injuries through earlier intervention, improved surgical techniques, and advanced medical care. Evidence-based practices for rehabilitation have been written and disseminated by researchers, thereby ensuring the best possible care for spinal cord patients across Canada and around the world. These results are a true testament to what can be accomplished when partnerships are forged and investments are leveraged toward a shared vision for the future. In 2007, the Rick Hansen Institute was established with the goal of being a catalyst for collaboration among spinal cord patients, researchers, clinicians and stakeholders across Canada and to advance the effectiveness, timeliness and quality of care of people with spinal cord injuries.
This model is now being extended to more than 70 sites worldwide – to develop new therapies and reduce the time required for research to be translated into real-life benefits. From day one, my team at the Rick Hansen Foundation has been dedicated to accelerating research for a cure for paralysis after a spinal cord injury, and creating an environment where best practices and new standards of accessibility can be developed and shared. In May of 2012, 2,500 international leaders and influencers will meet in Vancouver at the Interdependence 2012 Global Conference and Exposition to set the agenda for advancing spinal cord research and creating communities that are accessible to all. Our efforts must be focused, visionary and collaborative to support the impact of the world’s shift in population age and subsequent rise in disability. I truly believe we’re on the threshold of an exponential expansion of the boundaries of our knowledge. As I look to the future, I see a world where those newly injured as a result of spinal cord injuries walk away and the billion people on Earth living with various types of disabilities have equal opportunity to participate in, and contribute to, all aspects of their communities.
The HandTutor and its sister devices (ArmTutor, LegTutor, 3DTutor) have been in the forefront of spinal cord injury rehabilitation.
These innovative Tutor devices implement an impairment based program with augmented feedback and encourage motor learning through intensive active exercises. These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. The Tutor system also includes objective quantitative evaluations that provide the therapist information to customize the most suitable rehabilitation program to the patient’s ability. Currently part of the rehabilitation program of leading U.S. and foreign hospitals the Tutors are also used in clinics and at home through the use of telerehabilitation. The Tutors are suitable for children as well as adults.See www.HandTutor.com for more information.
Thursday, 17 November 2011
Congresswoman’s Recovery May Include HandTutor

On November 16, 2011 Carey Goldberg wrote the following for WBUR.ORG
I was having some personal trouble with the wall-to-wall coverage of the tortuous but remarkable recovery by Rep. Gabrielle Giffords, the Arizona Congresswoman who was shot in the head in January. From ABC to The Huffington Post to our own NPR, her husband, Mark Kelly, talked about her frustrations, her indomitable attitude and her plans to get back to work. The couple’s new book is called “Gabby: A Story of Courage and Hope.”
My trouble stemmed from the many survivors of severe brain injury that I saw 20 years ago after my mother was in a terrible car accident. They sat in their beds or in wheelchairs and stared blankly, for hours on end. Taped on the walls of their rooms were photos of the vibrant people they used to be; now their bodies seemed like leftover shells with the essence removed. There was no question of courage. They weren’t present enough to be brave. There was hope — isn’t there always hope? But I came to wonder whether the stories of recovery “miracles” might not do more harm than good in some ways, because they made it even harder for families like ours to accept the reality that in fact, in a case like my mother’s, there could be no recovery — ever. Not a single word. Not even a single hand-squeeze.
I took my troubles to Dr. Ross Zafonte of Spaulding Rehabilitation Hospital, an expert on rehabilitation for traumatic brain injury and chair of Harvard Medical School’s rehabilitation department. Might it not be problematic, I asked, that in the public mind, Gabrielle Giffords will now be the image of brain injury, when her recovery is actually so extraordinary? His response, lightly distilled:
“I would comment that the extent of the injury, the type — as well as its mechanisms — produce variability in the injury. That fact impacts our potential for recovery, as well as our own gender, and genetics.
In other words, if I’m in an auto accident, that might be different from a blast-related military injury, different from a fall, and that has so much to do with the type of injury and the potential for recovery. We have gotten very good, in the last 15 to 20 years, at maximizing motor and cognitive potential, especially motor potential.
The variability of the injury is one of its sentinel hallmarks. Two persons could fall off a mountain. They have the same kind of injury, the same kind of treatment, from neurosurgery to the same rehabilitation department, and one is very functional and returned to banking, and the other could be severely disabled.
The variability of the injury is one of its sentinel hallmarks.
The point is the personal variability: And then if we apply optimal acute and intermediate interventions, often now we get a Gabby Giffords; we get a Bob Woodward, who’s back at reporting and going all over the planet. It’s very much where and how and when. What we’re trying to do now in rehabilitation is further define the biology of that injury and recovery , and understand how we could manipulate it better.
So then what, I asked, is the message you hope that people take away from the Gabrielle Giffords story?
A message of hope. A message of persistence. A message of potential. A message that recovery and REHABILITATION is important. A message that we shouldn’t sell those issues short. We have so many people who are like that; her recovery is a very good one and we’re enthusiastic about it.
She still has some language issues, you can see. She still has some motor dysfunction on one side. But the reality is that we see these kinds of things nowadays on a regular basis. Not everybody recovers to that extent — that’s the problem. Particular areas of the brain are difficult for us to help recover.
Who does best?
People who have very focal injuries that are quickly operated on over a small area tend to do the best. People who are high-functioning at baseline also do better. Those who have very severe diffuse injuries that involve some of the connection areas and result in a disconnection syndrome probably face more challenges.
Even some of those persons, seen a year later, are ‘Wow!’ They have made a substantial recovery. It’s that perspective of time that people miss — looking at her from day 1 or day 2 to now — and that’s the big picture we all need to have. You may see someone early on and say, ‘Well, they don’t have much potential,’ when the reality is they do.
We’ve begun to understand the physiology of the disease — and it really is a disease — and how to manipulate things acutely. We’ve been able to cut down on people’s mortality over 20 years, and we’ve been able to gain insight into ways to help them recover their motor function. We have new ways that we teach people to walk; ways that we try to enhance the integration of their learning; ways that we try to improve their balance or their verbal output — though that one we struggle with more.
While I am not treating her it is clear that Gabby Giffords has aphasia, a language disorder. I think she’s going to undergo some further, very focused language therapy. I think they’re going to look at all the options. There’s no magic pill yet for aphasia but tremendous progress is being made.
The HandTutor and its sister devices (ArmTutor, LegTutor, 3DTutor) are FDA and CE certified and are being used in leading U.S. and foreign hospitals in their rehabilitation programs. They have had success in improving movement of the hand, wrist, elbow, knee, ankle, foot and other joints of the body following traumatic injuries. The Tutor devices have been effective for post stroke victims as well as for those suffering from brain injuries, Cerebral Palsy, spinal cord injuries , Apraxia, MS, Parkinsons and other movement disabilities. Intensive active exercise can reduce the rate of deterioration and this is what the ”Tutor” devices provide.
The Tutor system is also used in physical therapy clinics as well as the patient’s home with tele rehabilitation. The ”Tutors’‘ are suitable for adults and children. See www.HandTutor.com for more information.
Tutor System to Assist in Pediatric Rehabilitation

Diana Kraus and Dr. Martin Keller posted the following in STL Health and Fitness: Thursday, November 17, 2011 According to the National Center for Injury Prevention and Control, the most common cause of death in children ages 1-14 is injury. Given the vast numbers of injuries, more children die each year from this cause than cancer, infection, birth defects and heart disease combined. So, as a parent, where should you seek medical care if your child is injured? Data from the National Pediatric Trauma Registry show a three-fold increase in mortality of children with head injuries managed at adult centers rather than pediatric. Further, a study published in the Journal Trauma in 2007 indicates children who have suffered a traumatic injury who are treated by a pediatric trauma team have fewer operations to manage liver or spleen injuries, shorter lengths of stay, require transfusions, and the list goes on. Adult and pediatric trauma are reviewed by state or national governing organizations, but only pediatric centers must meet standards that are unique, comprehensive and most appropriate for children. After all, children are not just little adults. The regulations for a level 1 pediatric trauma center require that its specialists have received training in residencies and fellowships specific to children. This physician component in care is extremely important. Through a better understanding of the differences between a child and adult, in addition to improved survival, pediatric specialists will manage your child with fewer X-rays, transfusions and earlier return to function. Let’s say your 6-year-old falls off the jungle gym at home and hits his head. The baby-sitter reports that he was unconscious for 30 seconds and is now awake but sleepy and has bruising and abrasions to the side of his head. As a parent, you’re concerned and want him checked out immediately. If he is brought to a level 1 pediatric trauma center he will be first evaluated by physicians trained in pediatric emergency medicine and pediatric surgery/trauma. Level 1 pediatric trauma centers in the St. Louis area are St. Louis Children’s Hospital and Cardinal Glennon Children’s Medical Center. Mercy Children’s Hospital in St. Louis is a level 2 pediatric trauma center. A pediatric radiologist will use X-ray techniques, dosing and studies appropriate for children, understanding the normal variants which can be observed in the developing child. If he is admitted for a traumatic brain injury he will be cared for by pediatric neurosurgeons, pediatric intensivists and pediatric critical care nurses. As he improves, pediatric rehabilitation specialists, with pediatric trained physical and occupational therapists will be available. The Tutor system can be incorporated into the therapeutic program. From start to finish, his care will have been guided by physicians and staff with expertise and experience specific to the care of the injured child. This can mean the difference between walking out of the hospital in a week, or requiring months of rehabilitation. Numbers matter. As a parent with an injured child, the decision to seek care at a level 1 pediatric trauma center can make all the difference.
The new FDA and CE certified HandTutor, ArmTutor, LegTutor and 3DTutor have been developed to improve joint movement in brain and spinal cord injury victims. The Tutor devices are currently being used in leading U.S. and foreign hospitals as well as in physical therapy clinics and even in the patient’s home with tele rehabilitation. The Tutor devices also treat those suffering from MS, Parkinson’s, spinal cord injuries Apraxia among other disabilities. Intensive active exercise can reduce the rate of deterioration and this is what is provided with the Tutor devices.
The exercises are designed in the form of challenging games that are suitable for a wide variety of neurological and orthopedic injury and disease.The games challenge the patient to perform the exercise task to their best ability and to continue exercise practice and therefore provide a ”fun task” for children.
For those patients who are at home, both children and adults, the Tutor system is equipped with tele rehabilitation capability. See www.HandTutor.com for more information.
Wednesday, 16 November 2011
Joint Dislocation Rehabilitation Enhanced by ArmTutor

Drs.Katsumi Takase etal writing for the EUROPEAN JOURNAL OF ORTHOPAEDIC SURGERY & TRAUMATOLOGY report on a research project involving joint dislocation.
Generally, the surgical treatment for traumatic acromioclavicular joint dislocation is recommended for type 5 according to Rockwood’s classification. We believe that anatomical restoration of coracoclavicular ligament could best restore the function of the acromioclavicular joint. We attempted to correctly reconstruct the anatomy of the coracoclavicular ligament (trapezoid and conoid ligaments) in which the ipsilateral palmaris longus tendon and Endobutton were used as the reconstructing ligament and fixation material, respectively.
They conducted a cross-sectional study. The subjects were 16 patients (15 men and one woman). The mean age at the time of the surgery was 38.6 years. The mean time of the surgery from the injury was 16.3 days. The mean duration of postoperative follow-up was one year and 5 months.
The Results they found were that the reduction in the acromioclavicular joint was complete in 10 of 16 patients. Meanwhile, the subluxation that represented less than 5 mm superior translation of the clavicle, occurred only in 5, that represented 5–10 mm superior translation in none, and the complete dislocation occurred in one patient. Concerning the range of motion, mean forward flexion was 171°, mean abduction was 165°, mean internal rotation was Th11, and mean horizontal adduction was 132°. Pain, fatigues on the shoulder girdle, and impairments with shoulder motion on the affected side disappeared one month after surgery.
The conclusion they arrived at was that although it requires excision of the ipsilateral palmaris longus for graft, we believe that anatomical restoration of both coracoclavicular ligaments could best restore the function of the acromioclavicular joint.
Joint dislocation rehabilitation therapy can be greatly enhanced through the use of the newly developed ArmTutor.
The ArmTutor™ system has been developed to allow for functional rehabilitation of the upper extremity. The system consists of an ergonomic wearable arm brace and dedicated rehabilitation software. The ArmTutor™ system allows for a range of biomechanical evaluation including speed, passive and active range of motion and motion analysis of the upper extremity. Quantitative biomechanical data allow for objective evaluation and rehabilitation treatment follow up. The ArmTutor™ rehabilitation concept is based on performing controlled exercise rehabilitation practice at a patient customized level with real time accurate feedback on the patient’s performance. The exercises are designed in the form of challenging games that are suitable for a wide variety of neurological and orthopedic injury and disease.The games challenge the patient to perform the exercise task to their best ability and to continue exercise practice.
The ArmTutor™ allows for isolated and a combination of elbow and three directional shoulder treatment. The system provides detailed exercise performance instructions and precise feedback on the patients exercise performance. Controlled exercise of multijoints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks.
The ArmTutor™ system together with its sister devices (HandTutor, LegTutor, 3DTutor) is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. See www.HandTutor.com for more information.
Injured Libyans Assisted by Tutor System

Martine Powers writing for The Globe on November 11, 2011 reports on a story about veterans of the recent Libyan uprising.
Marwan Mafud, 22, wasn’t a soldier. During the Libyan revolution, he was a college student who used his car to bring medical supplies to rebel troops.
Though he was a civilian, government soldiers pulled him over. They spotted a rebel flag in his car and dragged him to the ground. They beat him, fracturing his skull and breaking his right hand. They called him a rat. Then, the soldiers demanded that he declare that Moammar Khadafy was god.
Mafud refused. “Allahu akbar,’’ he said. God is great.
Mafud is one of 22 Libyan men who were flown out of their country and brought to Spaulding Hospital North Shore in Salem almost two weeks ago to receive rehabilitation care for their
war injuries. The Libyan National Transitional Council organized the transfer, with the help of the US State Department. The patients, from different parts of Libya and ranging in age from 16 to 49, arrived with injuries of all kinds: bullet wounds, broken bones, nerve and spinal damage.
Spinal damage is one of many disabilities treated by the newly created Tutor system. Consisting of the HandTutor, ArmTutor, LegTutor and 3DTutor these devices are designed to improve motor, sensory and cognitive impairments through intensive active exercises with augmented feedback.
These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. The Tutor system also includes objective quantitative evaluations that provide the therapist information to customize the most suitable rehabilitation program to the patient’s ability. Currently part of the rehabilitation program of leading U.S. and foreign hospitals the Tutors are also used in clinics and at home through the use of telerehabilitation. The Tutors are suitable for children as well as adults.See www.HandTutor.com
Tutor System Aids in Motor Weakness Rehabilitation

Drs. O. L. Kim and S. H. Kim of the College of Medicine, Yeungnam University, Taegu, Korea write in the November 14,
2011 issue of Archives of Neurology about the fact that many studies have attempted to elucidate the causes of motor weakness in patients with traumatic brain injury (TBI). Most of these studies have focused on the specific cause of motor weakness. However, little is known about the classification and elucidation of the causes of motor weakness in consecutive patients with TBI.
To attempt to classify with diffusion tensor imaging the causes of motor weakness in patients with TBI by conducting an analysis of the injury mechanism of the corticospinal tract (CST).a study was conducted.
The study took place in the rehabilitation department of a university hospital. They recruited 41 consecutive patients who showed motor weakness among patients with TBI admitted for rehabilitation.
They classified the causes of weakness according to the injury mechanism of the CST on diffusion tensor imaging and
found that the injury mechanisms of the CST were classified as follows, in order: diffuse axonal injury, 24 patients (58.5%); traumatic intracerebral hemorrhage, 9 patients (21.9%); transtentorial herniation, 6 patients (14.6%); and focal cortical contusion, 4 patients (9.8%). In patients with diffuse axonal injury, the mean number of lesions composing CST injury was 3.6 (range, 2-6) and CST injury locations were as follows: the pons (61%), the cerebral peduncle (50%), the medulla (40%), the posterior limb of the internal capsule (17%), and the corona radiata (13%).
The conclusions they found were that diffusion tensor imaging was useful in elucidation and classification of the causes of motor weakness resulting from CST injury in patients with TBI.
When the Tutor system enters the “rehabilitation picture” the potential results are markedly improved. Used for SCI as well as brain injury, Parkinson’s disease, MS, CP, stoke, upper and lower extremity surgeries, Radial and Ulnar nerve injuries, Complex Regional Pain Syndrome and other disabilities the Tutor system implements an impairment based rehabilitation program with augmented feedback and encourages motor learning through intensive active exercises.
The newly developed Tutors and its component devices (HandTutor, ArmTutor, LegTutor, 3DTutor) have become a key system in neuromuscular rehabilitation and physical therapy. These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. The Tutor system also includes objective quantitative evaluations that provide the therapist information to customize the most suitable rehabilitation program to the patient’s ability. Currently part of the rehabilitation program of leading U.S. and foreign hospitals the Tutors are also used in clinics and at home through the use of telerehabilitation. The Tutors are suitable for children as well as adults.See www.HandTutor.com
Monday, 14 November 2011
Constraint Induced Movement Therapy Enhanced with the Tutor Sytem

Edward Taub, PhD; Gitendra Uswatte, MA; Rama Pidikiti, MD of the Physical Medicine and Rehabilitation Service, Birmingham Department of Veterans Affairs Medical Center, Birmingham, Alabama,U.S.A. discuss the much touted new technique called Constraint-Induced Movement Therapy or CI Therapy.
A new family of rehabilitation techniques, termed Constraint-Induced Movement Therapy or CI Therapy, has been developed that controlled experiments have shown is effective in producing large improvements in limb use in the real-world environment after cerebrovascular accident (CVA). The signature therapy involves constraining movements of the less-affected arm with a sling for 90% of waking hours for 2 weeks, while intensively training use of the more-affected arm. The common therapeutic factor in all CI Therapy techniques would appear to be inducing concentrated, repetitive practice of use of the more-affected limb. A number of neuroimaging and transcranial magnetic stimulation studies have shown that the massed practice of CI Therapy produces a massive use-dependent cortical reorganization that increases the area of cortex involved in the innervation of movement of the more-affected limb. The CI Therapy approach has been used successfully to date for the upper limb of patients with chronic and subacute CVA and patients with chronic traumatic brain injury and for the lower limb of patients with CVA, incomplete spinal cord injury, and fractured hip. The approach has recently been extended to focal hand dystonia of musicians and possibly phantom limb pain.
As an example of a disability where the CI therapy can be used: Cerebrovascular accident (CVA) is the leading cause of disability in the United States. A recent study indicates that the number of CVAs may be dramatically higher than was previously thought to be the case. The total number is now estimated to be approximately 730,000 every year and the data suggest that this may be an underestimate. Moreover, more than half of these individuals are left with motor disability. There seems little doubt that the number of CVA survivors will increase greatly as the population progressively ages over the next 50 years; a recent projection is that the prevalence of CVA will more than double during this period . A 1993 estimate placed the annual costs of CVAs at $30 billion, of which $17 billion were direct medical costs and $13 billion were indirect costs due to lost productivity . The American Heart Association estimates that the current direct and indirect costs of CVA are $43.3 billion per year . CVAs are a particular problem for the VA because of the large population of World War II and Korean War veterans who are now in the age ranges where CVAs are most frequent; in fiscal year 1997 the national VA system had 22,000 admissions for an acute CVA . The consequent motor deficits that veterans sustain result in very large costs to the VA and the Federal Government. The reduction of CVA-related disability thus represents a high VA and national health care priority.
At present, there is little experimental evidence available indicating that physical and occupational therapy is effective for patients with chronic CVA. The literature is even equivocal on the value of physical rehabilitation for sub-acute patients–see literature reviews from the past 10 years . In the Winter 1998 issue of the journal Topics in Stroke Rehabilitation devoted to “Functional Implications of Upper Extremity Management,” there was minimal discussion of specific therapeutic approaches to improving upper limb function, even though the title suggests that this would be a major, if not the main, topic covered. The small amount of material on upper limb treatment in that special issue may be a meaningful index of the fact that there are few empirically validated treatments to discuss at this time. The special issue did not review Constraint-Induced (CI) Movement Therapy, the treatment approach discussed in this article. The only literature review recent enough to evaluate published studies on CI Therapy cites it as being only one of three treatments for which there is empirical evidence of clinical efficacy and the only one to: 1) be supported with evidence from controlled randomized studies, and 2) have been shown to be effective for the upper limb . Moreover, CI Therapy does not involve medications or side effects, and there are no significant risks.
CI Therapy consists of a new set of rehabilitation techniques that data from controlled, randomized studies have indicated can substantially reduce the motor deficit of the more-affected limbs of many patients with chronic CVAs. The therapeutic effect has been demonstrated to transfer from the clinic to the real world; patients show increases in the daily use of their more-impaired limbs that are maintained, in the most powerful intervention, for at least 2 years after treatment . For the upper limb, the therapy involves inducing use of the more-affected limb for a target of 90 percent of waking hours by employing one of several methods for constraining or reducing use of the less-affected limb for 2 or 3 weeks. Concentrated, repetitive training of the more-affected limb is given daily for 6 hours, interspersed with 1 hour of rest, for each of the weekdays over the 2- or 3-week period (i.e., massed practice). The upper limb intervention has been tested to date with all but what we estimate to be the lowest functioning 25 percent of the chronic CVA population with significant residual motor deficit. For the lower limb, a somewhat different approach is used that does not involve less-affected limb restraint, but does include massed practice of functional lower limb activities (see below). This article reviews the development of CI Therapy from basic research with monkeys to its application to persons with CVA with upper limb deficits and its extension to the treatment of upper limb deficits in traumatic brain injury and lower limb deficits in persons with CVA, spinal cord injury, and hip fracture. The article also describes research suggesting that cortical reorganization is a possible mechanism that accounts for the persistent therapeutic effect of our intervention and discusses further rehabilitation applications that have emerged from this finding. The Tutor system has been developed to improve functional outcomes in physical rehabilitation with interactive rehabilitation exercises that include working with the Constraint-Induced Movement technique. CVA is but one of the health issues that can be helped by the Tutor system. Others include Parkinson’s, Brain and spinal cord injuries, upper and lower limb surgeries, CP, MS, Radial and Ulnar nerve injuries, development co-ordination disorders, Brachial Plexus injuries and Complex Regional Brain Syndrome.
The newly developed HandTutor and its sister devices (ArmTutor, LegTutor, 3DTutor) have become a key system in neuromuscular rehabilitation and physical therapy. These innovative devices implement an impairment based program with augmented feedback and encourage motor learning through intensive active exercises. These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. The Tutor system also includes objective quantitative evaluations that provide the therapist information to customize the most suitable rehabilitation program to the patient’s ability. Currently part of the rehabilitation program of leading U.S. and foreign hospitals the Tutors are also used in clinics and at home through the use of telerehabilitation. See www.handtutor.com
Complex Regional Pain Syndrome Treatment Involves Tutor System

Complex regional pain syndrome (CRPS) is a chronic pain condition that is believed to be the result of dysfunction in the central or peripheral nervous systems. Typical features include dramatic changes in the color and temperature of the skin over the affected limb or body part, accompanied by intense burning pain, skin sensitivity, sweating, and swelling.CRPS I is frequently triggered by tissue injury; the term describes all patients with the above symptoms but with no underlying nerve injury. Patients with CRPS II experience the same symptoms but their cases are clearly associated with a nerve injury., CRPS can strike at any age and affects both men and women, although most experts agree that it is more common in young women., The key symptom of CRPS is continuous, intense pain out of proportion to the severity of the injury (if an injury has occurred), which gets worse rather than better over time. CRPS most often affects one of the extremities (arms, legs, hands, or feet) and is also often accompanied by:, “burning” pain, increased skin sensitivity, changes in skin temperature: warmer or cooler compared to the opposite extremity, changes in skin color: often blotchy, purple, pale, or red, changes in skin texture: shiny and thin, and sometimes excessively sweaty, changes in nail and hair growth patterns, swelling and stiffness in affected joints, motor disability, with decreased ability to move the affected body part, Often the pain spreads to include the entire arm or leg, even though the initiating injury might have been only to a finger or toe. Pain can sometimes even travel to the opposite extremity. It may be heightened by emotional stress., The symptoms of CRPS vary in severity and length. Some experts believe there are three stages associated with CRPS, marked by progressive changes in the skin, muscles, joints, ligaments, and bones of the affected area, although this progression has not yet been validated by clinical research studies., Stage one is thought to last from 1 to 3 months and is characterized by severe, burning pain, along with muscle spasm, joint stiffness, rapid hair growth, and alterations in the blood vessels that cause the skin to change color and temperature., Stage two lasts from 3 to 6 months and is characterized by intensifying pain, swelling, decreased hair growth, cracked, brittle, grooved, or spotty nails, softened bones, stiff joints, and weak muscle tone., In stage three the syndrome progresses to the point where changes in the skin and bone are no longer reversible. Pain becomes unyielding and may involve the entire limb or affected area. There may be marked muscle loss (atrophy), severely limited mobility, and involuntary contractions of the muscles and tendons that flex the joints. Limbs may become contorted., Doctors aren’t sure what causes CRPS. In some cases the sympathetic nervous system plays an important role in sustaining the pain. The most recent theories suggest that pain receptors in the affected part of the body become responsive to a family of nervous system messengers known as catecholamines. Animal studies indicate that norepinephrine, a catecholamine released from sympathetic nerves, acquires the capacity to activate pain pathways after tissue or nerve injury. The incidence of sympathetically maintained pain in CRPS is not known. Some experts believe that the importance of the sympathetic nervous system depends on the stage of the disease., Another theory is that post-injury CRPS (CRPS II) is caused by a triggering of the immune response, which leads to the characteristic inflammatory symptoms of redness, warmth, and swelling in the affected area. CRPS may therefore represent a disruption of the healing process. In all likelihood, CRPS does not have a single cause, but is rather the result of multiple causes that produce similar symptoms., CRPS is diagnosed primarily through observation of the signs and symptoms. But because many other conditions have similar symptoms, it can be difficult for doctors to make a firm diagnosis of CRPS early in the course of the disorder when symptoms are few or mild. Or, for example, a simple nerve entrapment can sometimes cause pain severe enough to resemble CRPS. Diagnosis is further complicated by the fact that some people will improve gradually over time without treatment., Since there is no specific diagnostic test for CRPS, the most important role for testing is to help rule out other conditions. Some clinicians apply a stimulus (such as touch, pinprick, heat, or cold) to the area to see if it causes pain. Doctors may also use triple-phase bone scans to identify changes in the bone and in blood circulation., The prognosis for CRPS varies from person to person. Spontaneous remission from symptoms occurs in certain people. Others can have unremitting pain and crippling, irreversible changes in spite of treatment. Some doctors believe that early treatment is helpful in limiting the disorder, but this belief has not yet been supported by evidence from clinical studies. More research is needed to understand the causes of CRPS, how it progresses, and the role of early treatment., Because there is no cure for CRPS, treatment is aimed at relieving painful symptoms so that people can resume their normal lives. One of the therapies that is often used is, Physical therapy: A gradually increasing exercise program to keep the painful limb or body part moving may help restore some range of motion and function. This is where the Tutor System plays an integral part. The newly developed HandTutor and its sister devices (ArmTutor, LegTutor, 3DTutor) have become a key system in neuromuscular rehabilitation and physical therapy. These innovative devices implement an impairment based program with augmented feedback and encourage motor learning through intensive active exercises. These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. The system also includes objective quantitative evaluations that provide the therapist information to customize the most suitable rehabilitation program to the patient’s ability. Currently part of the rehabilitationprogram of leading U.S. and foreign hospitals the Tutors are also used in clinics and at home through the use of telerehabilitation. see www.HandTutor.com
Pediatric Rehabilitation in Children with Cerebral Palsy Assisted by LegTutor

J. G. BECHER, MD, PhD of the Department of Rehabilitation Medicine of the VU University Medical Centre, Amsterdam,The Netherlands gives an overview of Pediatric CP and its treatment.
ABSTRACT
Cerebral palsy (CP) is the most common physical disability in childhood. The motor impairment syndrome is obligatory for the diagnosis, but a broad range of neurological deficits can be present as well. Professionals in pediatric rehabilitation are faced with a diversity of problems in the child and family (physical, psychological, communicative, and social), so a multidisciplinary approach for treatment is needed. The International Classification of Functioning offers a framework for team management in the treatment of children with CP. Based on this concept, an instrument for team conferences, the Children’s Rehabilitation Activities Profile is described. This instrument can be used for systematic evaluation of the needs of the children and parents, the total development and evaluation of the goals of rehabilitation on the level of activities. In children with CP, three main kinds of motor disorders are seen: spastic paresis; ataxic paresis, and dyskinetic paresis. In the most common disorder, spastic paresis, many different impairments of muscle function are described. Spasticity is only one of the components of a spastic paresis. The clinical consequences of these differences are discussed. In children with walking ability, the walking pattern is related to the functional prognosis of ambulation at adulthood. A classification of walking patterns is presented that can be used as a framework for treatment programs.
Cerebral palsy (CP) is an umbrella term covering a group of nonprogressive–but, in time, often changing–motor impairment syndromes secondary to lesions or anomalies of the immature brain.1 Onset usually occurs before the first birthday. CP is the most common physical disability in childhood; the incidence was stabilized in the nineties at around 2-2.5per 1000 live births.2
Although the motor disorder is the most striking symptom, many other pediatric and neurological impairments are associated with CP, such as failure to thrive caused by feeding problems or constipation, seizures, visual and auditory impairments, mental retardation, speech impairments, such learning deficits as dyslexia and nonverbal learning disability, and behavioral impairments.
GENERAL MANAGEMENT
Treatment of children with CP requires a long-term process during growth by a multidisciplinary team, focusing on all developmental aspects of the child and planning interventions in relation to the most urgent needs of the child and the family. The long-term goal is the optimal functioning in adulthood.3 The organization of the health care for children with CP is very heterogeneous within and among countries. Recently, minimal acceptable standards have been described. Pediatricians, pediatric orthopaedic surgeons, pediatric neurologists, and, rather uniquely in the Netherlands, pediatric physiatrists are involved in the multidisciplinary treatment of children with CP. The International Classification of Functioning (ICF) model offers a framework for a multidisciplinary, need-oriented team approach. Based on this model, the Rehabilitation Activities Profile for children (Children’s RAP) has been developed. This is an instrument for team communication on the level of abilities and so avoids the use of jargon. The goals of treatment also require description of the level of abilities. Long-term (e.g., the child will walk independently without walking aids, following education in a primary school) and short-term goals (e.g., the child can sit on a chair for 60 seconds without support) need to be described in a measurable way. In this way, evaluation of the goals in the team conferences is possible, and the results of treatment are clear for all team members as well as for the parents.
MEDICAL MANAGEMENT
Prognosis of movement abilities can be made in the second to third year of life and is strongly related to the kind and localization of the motor disorder and the mental status of the child. There are three main types of motor syndromes: spastic paresis, ataxic paresis, and dyskinetic paresis.
Spastic paresis is characterized by a posture- and movement-dependent tone regulation disorder. The clinical symptoms are the loss or absence of tone in lying, and increase in tone in sitting, standing, walking, or running, depending on the degree of involvement. Spastic paresis is the most common motor disorder (83%).
In patients with ataxic paresis, impairments of equilibrium and coordination are dominant. There are hypermetric movements in the extremities, and tremor and titubations can be present. Only 4% of children with CP have a mainly ataxic paresis, often with some signs of spasticity in the legs. The time course of obtaining walking ability is delayed in comparison with spastic paresis, but most children achieve walking ability, at least with a walking aid.
Dyskinetic paresis can be divided into the hyperkinetic (athetoid) type, characterized by involuntary movements, most pronounced in the face and extremities, which are present even at rest, and the dystonic type, characterized by slow powerful contractions of agonist and antagonist of movement simultaneous, locally or with total body involvement. In time, a hyperkinetic type of movement can change into a dystonic type, and combinations are also possible. The development of head and trunk balance is delayed. Some children achieve walking ability even at the age of 10 years. Dyskinetic paresis is seen in 12% of children with CP.
For the proper treatment of children with CP, the classification of the kind of motor disorder is crucial. The surgical and orthotic management in children with dyskinetic or ataxic paresis is completely different from that of children with spastic paresis. Because the spastic paresis is the most common motor syndrome, this article will focus on that motor disorder.
The motor disorder can also be classified in regard to the localization: hemiplegia is defined as a unilateral involvement (33%); diplegia as a bilateral involvement, in which only the lower extremities are involved or the lower extremities are more involved than the upper extremities (44%); quadriplegia (or tetraplegia) is defined as a bilateral involvement, in which the upper extremities are equal or more involved than the lower extremities (6%). This classification is unambiguous and easy to use in clinical practice. [Classifications using the presence of muscle impairment of the upper extremities (paraparesis if no involvement of the upper extremities, diplegia with involvement of the upper extremities) or bulbar involvement (diplegia without bulbar involvement, quadriplegia with bulbar involvement) can cause confusion. These signs can be present only slightly, so it is difficult in clinical practice to set limits for the classification paraparesis, diplegia, and quadriplegia.] According to this classification, the functional prognosis of independent walking ability (with or without walking aids) can be set: 100% of the hemiplegic children, 85% of the diplegic children, based on the ability to put weight on the hands while prone at 18 months and a short sit at the age of 24 months, and none of the quadriplegic children will achieve independent walking ability in adulthood. The Gross Motor Function Classification System (GMFCS) is an instrument for early classification the severity of the motor disorder.
CLASSIFICATION OF IMPAIRMENT IN MUSCLE FUNCTION IN SPASTIC PARESIS
About 80-90% of the children have spastic paresis as the motor disorder. However, with regard to the impairment of muscle function, a variety of clinical symptoms can be distinguished. Several terms have been used in the literature to describe the different symptoms of spastic paresis, and the same terms are often defined differently. The term “spasticity” is often used for all kinds of motor disorders or for all signs of a spastic paresis. Because a proper description of the different symptoms is needed for selection of patients for a specific therapy, conventions about terminology are needed. The following classification is according to the actual insight.
In spastic paresis, three sets of symptoms can be distinguished: impairment of muscle activation; impairment of muscle stiffness; and impairment of muscle length.
IMPAIRMENT OF MUSCLE ACTIVATION
Impairment of muscle activation can be divided into deficit symptoms and excess symptoms.
Deficit symptoms are caused by the reduction of voluntary muscle function. In the case of mild involvement, only loss of dexterity of movement, diminished ability to perform fast alternating movements and enhanced fatigability are present. In more severe involvement, the patient can perform only synergistic voluntary movements and the level of force is reduced. The lowest level of motor control is voluntary movement in a general flexion (mostly present in the upper limbs) or extension pattern (mostly present in the lower limbs). Synergistic voluntary movements are also described as “loss of selective motor control.” In spastic paresis, the influence of posture is also increased. For instance, it is much easier for most patients to bend the hip in a sitting position than in a standing position. For that reason, it is not rational to use the Medical Research Council scale for grading the force of muscles when synergies of muscle movements are present.
Excess symptoms reflect the presence of abnormal muscle activity. Clinically, the presence of abnormal muscle activity can be noticed either during passive joint movements, while the patient is in maximal relaxation, or while the patient is performing motor tasks.
Passive Movement
During (very) slow passive movements, muscle tone can be examined. Some patients show a raised muscle tone during a very slow passive stretch (hypertonia defined as a non-velocity-dependent resistance to passive stretch). This increased resistance could be caused by a continuous activation of the stretched muscle (tonic stretch reflex activity).
During fast passive movements, the presence of spasticity, defined as the velocity-dependent resistance to passive stretch, can be examined. If only a catch (clasp-knife symptom) can be noticed, the spasticity is mild. In more severe spasticity, a clonus in the muscle or a marked increase in resistance can be evoked. Hyperreflexia of tendon jerks, abnormal cutaneo-muscular reflexes (such as Babinski’s response) are also excess symptoms.
When performing motor tasks, three other features of involuntary muscle activation can be present: mirror movements can be present in patients with a hemiplegia or asymmetric diplegia: strong voluntary contraction of a muscle on the unaffected side evokes contractions in the same muscle on the opposite side; involuntary synergies can arise during the performance of a motor task. For example, the occurrence of a flexor synergy in the arm of hemiplegic patients when walking; postural reflexes cause involuntary muscle activity during the performance of a motor task (e.g., the clawing of the toes when walking). The muscle contractions develop gradually during walking.
Active (Voluntary) Movement
During active movement, co-contraction of the antagonist is also an excess symptom. Clinically, co-contraction can sometimes be observed as a paradoxical movement. For instance, the patient is asked to extend the elbow, but a flexion movement takes place: the co-contraction of the flexors is more powerful than the contraction of the extensors of the elbow. There is no relationship between the presence of co-contraction during voluntary movement and spasticity during passive movement. The amount of co-contraction in repetitive movements of the ankle is significantly lower on the hemiplegic side than on the unaffected side.
IMPAIRMENT OF MUSCLE STIFFNESS
Clinically, increased muscle stiffness (defined as hypertonia) can be observed during slow passive stretch of a muscle after maximal relaxation. It is important to choose a posture for the patient in which maximal relaxation can be achieved (i.e., lying supine, flexion-abduction-exorotation in the hip and flexion in the knee will relax the triceps surae muscle). Without electromyographic activity, hypertonia can be caused by changes in the biomechanical properties of the muscle.
IMPAIRMENT OF MUSCLE LENGTH
The development of muscle shortening is a well-known phenomenon in clinical practice. It is unclear why muscle shortening is present in some patients and not in others. A neurological growth disturbance has been postulated. Because muscle shortening takes place in the pattern of movement, a relation between gait pattern and muscle shortening seems probable.
The clinical consequences of this classification are evident: treatment of spasticity can improve only functional problems caused by spasticity, not by other such impairments as postural reflexes, hypertonia, or muscle shortening. This is crucial, for instance, for selection of patients for a specific therapy, such as prescription of ankle foot orthoses or selective dorsal rhizotomy.
CLASSIFICATION OF GAIT PATTERN
In children with CP, the classification of gait pattern can be used to determine developmental risks, to forecast walking ability in time, and to define therapeutic measures, such as orthotic treatment or surgery. For hemiplegic patients, four kinds of gait patterns are recognized. The following classification can be used for both hemiplegic and diplegic patients. Diplegic patients can show different patterns for each leg.
Type 1: Insufficient Foot Lift in Swing
In children affected only mildly, the main problem in walking is insufficient foot lift in mid-swing and forefoot landing at initial contact. In general, insufficient activity in the tibialis anterior and/or shortening of the gastrocnemius muscle is the cause of this gait pattern.
Type 2: Knee (Hyper)Extension in Midstance without Heel Rise
More severely affected children show, besides the insufficient foot lift in mid-swing, knee extension or hyperextension after initial contact instead of knee flexion, without heel rise in midstance. This is caused by a premature activation of the triceps surae muscle. The forefoot landing may be caused not only by insufficient foot lift but also by incomplete knee extension in terminal swing due to insufficient selective motor control (in terminal swing, hip flexion must be combined with a knee extension movement.
Type 3: Knee (Hyper)Extension in Midstance with Heel Rise
This gait pattern is similar to type 2, but heel rise takes place in midstance. A higher degree of abnormal activation of the triceps surae muscle is present. Prolonged activation of the vastus lateralis muscle can be present as a sign of insufficient power of the gastrocnemius muscle in terminal stance. In that case, the risk of development of a gait type 4 is present.
Type 4: Knee Flexion in Midstance with Heel Rise
In severely affected children, a gait pattern characterized by hip and knee flexion in midstance can be present. This gait pattern can be caused by strong abnormal activity (with or without muscle shortening) of the gastrocnemius and hamstring muscles or by abnormal activity of the psoas and hamstring muscles. The former situation has a better functional prognosis than the latter. These children are at high risk of developing shortening of the psoas, hamstring, and gastrocnemius muscles, and, in later stages, flexion contractures in hip and knee joints. Because this gait pattern is very energy-consuming, deterioration in (pre)puberty can be expected.
Type 5: Knee Flexion in Midstance without Heel Rise
The worst pattern of gait is a gait pattern with flexion of the hip and knee in midstance without heel rise. Insufficient power of the gastrocnemius muscle must be present. Often, it is caused by previous gastrocnemius surgery or Achilles tendon lengthening, but it can also develop spontaneously. If a change of gait pattern in bilateral involvement, at least into type 4 gait pattern, cannot be reached, loss of walking ability can be expected in puberty.
Besides these gait patterns, foot deformation can be present (varus or valgus). Increased homolateral trunk movements or pelvic drop of the contralateral leg in midstance are signs of weakness of the hip abductors. Also, endorotation adduction motion in terminal swing can be present, in severe cases resulting in rubbing of the knees. This can be caused by shortening or abnormal activity of the medial hamstrings. Persistent adduction in stance and swing can be caused by shortened hip adductors, endorotation by increased hip anteversion and endorotation contractures. Exorotational or endorotational foot progression angles can be caused by hip rotational contractures or rotational deformities of the femur or tibia. Insufficient foot clearance in preswing can be related to insufficient hip and knee flexion or abnormal stretch reflex activity (and shortening) of the rectus femoris muscle.
All these aspects of the gait pattern must be taken into account for making a plan for improvement of gait. The task of the medical specialist is to coordinate the multidisciplinary treatment of children with CP. Setting long-term goals on the level of abilities is the major task of the team. The medical specialist must determine the functional possibilities of the child and the risks for deterioration during growth. The medical treatment should take place within a whole treatment program, taking into account all aspects of development of the child and the possibilities of its environment. It is a challenging task for teams specializing in the treatment of children with CP.
CONCLUSION
In children with CP, a complex of neurological impairments and developmental risks with regard to their physical, psychological, and social development can be present. Pediatric rehabilitation is a complex process, facing all these problems. First, the diagnosis and functional prognosis of the child with regard to movement abilities, cognition, and communication must be determined. A multidisciplinary treatment approach is needed. A tool for team conferences, based on the model of the ICF, is presented. Because the motor impairment is the main interest of medical treatment, classification of the motor syndromes and impairment of muscle functions are described. Finally, a classification of gait patterns in relation to the degree of involvement for patients with a spastic paresis is described. This classification can be used to set the prognosis of ambulation and the kind of interventions needed to optimize the walking ability.
The LegTutor has shown to be helpful in the rehabilitation treatment of children suffering from CP.
The LegTutor™ system has been developed to allow for functional rehabilitation of the lower extremity. The system consists of an ergonomic wearable leg brace and dedicated rehabilitation software. The LegTutor™ system along with its sister devices (HandTutor, ArmTutor, 3DTutor) allows for a range of biomechanical evaluation including speed, passive and active range of motion and motion analysis of the lower extremity. Quantitative biomechanical data allow for objective evaluation and rehabilitation treatment follow up. The LegTutor™ rehabilitation concept is based on performing controlled exercise rehabilitation practice at a patient customized level with real time accurate feedback on the patient’s performance. The exercises are designed in the form of challenging games that are suitable for a wide variety of neurological and orthopedic injury and disease.
The games challenge and entertain the pediatric patient to perform the exercise task to their best ability and to continue exercise practice.
The LegTutor™ allows for isolated and a combination of knee and three directional hip treatment. The system provides detailed exercise performance instructions and precise feedback on the patients exercise performance. Controlled exercise of multi joints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks.
The LegTutor™ system is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. See www.HandTutor.com
.
Sunday, 13 November 2011
HandTutor Improves Cognitive Impairments of TBI Patients

Lana J. Ozen and Myra A. Fernandes of the Department of Psychology, University of Waterloo, Waterloo, Ontario, Canada as reported in the Archives of Clinical Neuropsychology discuss the fact that long-term persistent attention and memory difficulties following a mild traumatic brain injury (TBI) often go undetected on standard neuropsychological tests, despite complaints by mild TBI individuals. They conducted a visual Repetition Detection working memory task to digits, in which they manipulated task difficulty by increasing cognitive load, to identify subtle deficits long after a mild TBI. Twenty-six undergraduate students with a self-report of one mild TBI, which occurred at least 6 months prior, and 31 non-head-injured controls took part in the study. Participants were not informed until study completion that the study’s purpose was to examine cognitive changes following a mild TBI, to reduce the influence of “diagnosis threat” on performance. Neuropsychological tasks did not differentiate the groups, though mild TBI participants reported higher state anxiety levels. On their working memory task, the mild TBI group took significantly longer to accurately detect repeated targets on the task, suggesting that slowed information processing is a long-term consequence of mild TBI. Accuracy was comparable in the low-load condition and, unexpectedly, mild TBI performance surpassed that of controls in the high-load condition. Temporal analysis of target identification suggested a strategy difference between groups: mild TBI participants made a significantly greater number of accurate responses following the target’s offset, and significantly fewer erroneous distracter responses prior to target onset, compared with controls. Results suggest that long after a mild TBI, high-functioning young adults invoke a strategy of delaying their identification of targets in order to maintain, and facilitate, accuracy on cognitively demanding tasks.
The HandTutor, together with its sister devices (ArmTutor, LegTutor, 3DTutor) improves fine motor, sensory and cognitive impairments through intensive active exercises with augmented feedback for TBI patients.The HandTutor™ evaluates and treats finger and hand movement dysfunction through exercises that encourage extension/ flexion of the finger(s) and wrist.
The HandTutor™ system consists of a safe comfortable glove, with position and speed sensors that precisely record finger and wrist motion, and dedicated rehabilitation software. The ergonomic gloves come in five sizes for both right and left hands. The rehabilitation system employs the known concept of biofeedback to give occupational and physical therapists access to an affordable user friendly hand rehabilitation package. The HandTutor™ can also be used in combination with the 3DTutor™ for arm rehabilitation. The HandTutor™ is CE medical and FDA certified. See www.HandTutor.com
Tutor System Inclusion in Guide to Disability Fitness Training Effective

Jake Lawless says it’s a challenge for those with spinal cord injuries to get started in a fitness routine.
As a younger man, Jake Lawless would tell friends that if they had a car accident with him as a passenger, they had better kill him because he couldn’t bear to live his life in a wheelchair.
Then at 24, he fell off a roof and landed on his head. The injury left him a high functioning quadriplegic.
“My injury was my worst nightmare come true,” says Lawless, 38.
Lawless knew physical activity was the key to his recovery. He credits an intensive rehabilitation routine with helping him deal with his disability and learn to walk again, a skill he lost again after another accident destroyed his knee.
As reported in SPEC.COM November 12, 2011, now a peer support worker, Lawless teaches adults with spinal injuries of the value of staying fit. He notes the biggest challenge for many is finding out what to do.
That barrier has been knocked down by a new fitness guide developed by McMaster University researchers. It lists activities for people with spinal injuries, how much they should do each week, provides a weekly action plan and strategies to overcome obstacles.
“This helps people with spinal cord injuries get going,” says Kathleen Martin Ginis, a kinesiology professor.
Less than half of the estimated 86,000 Canadians with a spinal cord injury are physically active. While fitness is important for everyone, Martin Ginis notes that it is critical for people with disabilities who are at risk of further complications.
The leading cause of death for people with spinal injuries is chronic disease but little information is available on fitness.
“People with disabilities in general are forgotten when it comes to physical activity,” she says.
Lawless, who now lives in Ayr and is touring with the Rick Hansen relay, believes it provides vital information.
“The hardest part is starting,” he says, noting that the mental benefits are just as important as the physical.
“It’s critical for their quality of life,” agrees Bill Adair, executive director of the Canadian Paraplegic Association Ontario.
One of his staff members with a spinal injury started has lost 13 pounds in five months following the Mac program and has never felt better. “It has made a huge difference.”
Try these activities
Manual chair
• Wheel for fun and endurance
• Cycle using hand cycle or stationary bike
• Swim
• Build strength with a resistance band
• Lift weights, even cans and water bottles will do
• Rake the lawn or shovel snow
Power chair
• Use a movement therapy machine like the Tutor system. (See below).
• Swim with assistance
• Use an arm ergometer
• Do standing frame exercises
• Dance
• Curl
• Use cable pulleys
• Practise yoga, Pilates or Tai Chi
The Tutor system (which includes the HandTutor, ArmTutor, LegTutor and 3DTutor) not only provides intensive exercises for the physically challenged but makes it fun as well. The newly developed Tutor system improves fine motor, sensory and cognitive impairments through those exercises and includes augmented feedback as well.
The exercises are designed in the form of challenging games that are suitable for a wide variety of neurological and orthopedic injury and disease. The games challenge the patient to perform the exercise task to their best ability. Rehabilitation games allow the patient to exercise Range of Motion (ROM), speed and accuracy of movement.
The ArmTutor™ , for example, allows for isolated and a combination of elbow and three directional shoulder treatment. The system provides detailed exercise performance instructions and precise feedback on the patients exercise performance. Controlled exercise of multijoints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks.
The Tutor system is also used in rehabilitation therapy for victims of Parkinson’s disease, MS, CP, Upper and lower limb surgeries, brain and spinal cord injuries and other disabling illnesses. It is currently in use in many leading rehabilitation centers worldwide and has full FDA and CE certification. See www.HandTutor.com
Subscribe to:
Posts (Atom)