Tuesday 31 July 2012
Voluntary Exercises Better Than External Stimuli for Physical Rehabilitation
In the Journal of NeuroEngineering and Rehabilitation, July 2012 edition, Dr.Kyung-Lim Joa of the Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan, South Korea published the results of a study in which rehabilitation was evaluated by using voluntary movements as well as Functional Electrical Stimulation (FES).
Nineteen healthy male subjects were enrolled in the study. The study design included: a-voluntary contraction only, b-functional electrical stimulation (FES)-induced wrist extension only, and c-simultaneous voluntary and FES-induced movement. Brain activation was observed in all three modes.
The activated brain regions (number of voxels) of the MI, SI, cerebellum, and SMA were LARGEST DURING VOLUNTARY CONTRACTION ALONE and smallest during FES alone. SII-activated brain regions were largest during voluntary contraction combined with FES and smallest during FES contraction alone. The brain activation extent (maximum t score) of the MI, SI, and SII was LARGEST DURING VOLUNTARY CONTRACTION ALONE and smallest during FES alone.
The conclusions drawn were that voluntary contraction combined with FES may be more effective for brain activation than FES-only movements for rehabilitation therapy. In addition, voluntary effort is the most important factor in the therapeutic process.
As it is this is another proof that the patient recovering from and undergoing rehabilitation for affected limbs due to Parkinson’s, CP, MS, stroke, brain or spinal injuries amongst other diseases and surgeries should be using physical therapy solutions that encourage the patient to use his own strength and efforts while exercising more than outside stimuli via robots or electrical impulses. Such physical therapy products can be found in the TUTOR system.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been designed for just that type of intensive exercise. Consisting of comforatble and ergonomically designed gloves or braces, The TUTORs improve fine motor, sensory and cognitive impairments through intensive exercises with augmented feedback. The exercises are challenging and motivating and allow for repetitive training tailored to the patient’s own performance. In the case of the HANDTUTOR, for example, the glove has been designed to detect finger and wrist motion and has an open palmar surface to give maximum motor and sensory input. The glove comes in different sizes to allow evaluation and treatment of patients from age 5 and up.
One of the most cost effective rehabilitation devices currently in use in leading U.S. and European hospitals the TUTORs are fully certified by the FDA and CE. They can also be used in the patient’s home via telerehabilitaion. See WWW.MEDITOUCH.CO.IL for more information.
Monday 30 July 2012
First Use of Hand At Age 12
It has just been reported that Kyril, a 12 year old boy from Latvia can now do anything he wants with his right hand for the first time in his life. Kyril is one of a rare group of children that suffered from Brachial Plexus Palsy, a defect that occurs in one in 3-5,000 births that prevents normal movement of the hand. Most children learn to cope with it and 90 percent of them eventually are fine as the disability passes by 3 months of age. With Kyril it didn’t and he was sent to Israel where Dr. Mark Edelman, a pediatric orthopedist and the head of the pediatric orthopedic department at Rambam Medical Center in Haifa, operated on him and ”rearranged” his wrist and shoulder bone. In addition to that miracle Kyril was able to leave the hospital after only one day as the operation precluded the need for a plastic cast and other treatments.
For others who are not so lucky and are suffering from Cerebral Palsy and other disabling diseases getting the right type of physical therapy solution is critical in order to restore normal movement in the affected limb. Such a solution can be found in the TUTOR system. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been included in physical therapy programs at leading U.S. and European hospitals and rehabilitation facilities. These devices are ergonomically designed gloves and braces that have sensors to detect even the slightest movement on dedicated software they are connected to. The physical therapists then record and quantify this information and design a customized intensive exercise program with augmented feedback leading to enhanced rehabilitation for the patient.
The TUTOR system is suitable for children as well as adults and can be used at the patient’s home through telerehabilitation. The TUTORs are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.

Thursday 26 July 2012
Meaningful Task-Specific Training (MTST) Works With Stroke Rehabilitation
K.N. Arya etal of the Department of Neurology, CSM Medical University, Lucknow, India in a study published in Top Stroke Rehabilitation in the May/June 2012 edition discuss the following study they conducted.
One of the functional challenges in post stroke patients is the upper extremity motor deficit. The objective of this study was to evaluate the results of the ”meaningful task-specific training” (MTST) on upper extremity motor recovery during the subacute phase after a patient suffers a stroke.
The study was conducted as a randomized, controlled and double-blinded trial in the neurology department of a university hospital and occupational therapy unit of a rehabilitation facility. A sample of 103 people post stroke, was randomized into 2 groups (the MTST group had 51 participants and the standard training group had 52). Ninety-five of the participants completed the 8-week follow-up program. Participants were assigned to receive either the MTST or dose-matched standard training program based on the Brunnstrom stage and Bobath neurodevelopmental technique, 4 to 5 days a week for 4 weeks.
The results showed a positive improvement in the scores of the MTST group at post and follow-up assessments in comparison to the control group. In addition, statistically significant differences were observed in changes between the groups at post and follow-up assessment for FMA, ARAT, GWMFT, and MAL.
The conclusion drawn was that the MTST group produced statistically significant results as well as clinically relevant improvements in the upper extremity motor recovery of the patients who had had a subacute stroke.
When providing physical therapy solutions for upper extremity movement disorders the ARMTUTOR is one of the leading and most cost effective products available.
The ARMTUTOR™ has been developed to allow for functional rehabilitation of the upper extremity including the shoulder, elbow and wrist. The system consists of an ergonomic arm brace together with dedicated rehabilitation software. The ARMTUTOR™ system and its sister devices (HANDTUTOR, LEGTUTOR, 3DTUTOR) allows the physical and occupational therapist to report on and evaluate the patient’s functional rehabilitation progress and then to prescribe the correct customized and motivating intensive exercise practice to the manual rehabilitation therapy. Intensive repetition of movement is achieved through challenging games set to the patient’s ability. The system provides detailed exercise performance instructions and precise feedback on the patient’s efforts. Controlled exercise of multijoints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks. Telerehabilitation allows the recovering patient to continue his physical therapy at home. The system is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. See WWW.MEDITOUCH.CO.IL for more information.

Wednesday 25 July 2012
Parkinson’s Disease–Not This Population
In the northern part of Israel and in Syria there is a group of people called ”Druse”. A new study by the University of Haifa and the Carmel and Rambam Medical Centers in Israel has found that the Druse people have a much lower incidence of Parkinson’s disease (PD) than in other populations. In addition it was found that this group suffers less from Essential Tremor (ET). This despite that the Druse tend to intramarry, a fact that usually brings with it higher genetic disease rates.
Funded by the Israeli Ministry of Science and Technology the researchers found that the group is a “genetic nature reserve” since they have lived in the same general area for over 1,000 years and do not marry outsiders. Amongst the statistics is the fact that in the rest of the world ET affects an average of 4% of the poulation over 40 and PD an avaerage of 1.5%.
The study was conducted with 9000 Druse who were 51 or over and who live in the Galilee section of Israel. Blood samples were taken from those who suffered from any kind of tremor. Of the group only 27 had full tremors and 9 had PD. The researchers were surprised at the low at the low percentage for a group of people that practiced consanguinity (marrying cousins). Normally such a group would be more likely to get PD and ET. A previous survey, though, discovered that genetically 150 different genealogical lines made up the community. This suggested to the researchers that because of so many lines when the community was originally formed it prevented the increase in genetic diseases.
For those people who are not part of the Druse population Parkinson’s disease can be very debilitating. Fortunately there are physical therapy solutions that can offer some relief for PD symptoms. At the forefront is the HANDTUTOR.
The newly developed HANDTUTOR and its sister devices (LEGTUTOR, ARMTUTOR and 3DTUTOR) have become a key system in neuromuscular rehabilitation and physical therapy for Parkinson’s patients as well as those affected by brain/spinal cord injury and other upper and lower limb disabilities . These innovative devices implement an impairment based program with augmented feedback that encourages intensive practice and motor learning through active exercises. The exercises are challenging and motivating and allow for repetitive and intensive training tailored to the patient’s performance and motor, sensory and cognitive movement ability. Customized and simple but powerful rehabilitation software allows the physical and occupational therapist the ability to adjust the program and exercise difficulty to the patient’s movement level. The system also includes objective quantitative evaluations that allow the physiotherapist and his occupational therapist colleagues to report on the patient’s exercise progress.
Telerehabilitation features allow the patient to be supported by the physical rehabilitation team when he is at home. This ensures that the patient is motivated to do more practice between treatments by the therapists. The TUTOR system is suitable for children as well as adults. They are certified by the FDA and CE and are available for children as well as adults. See WWW.MEDITOUCH.CO.IL for more information.

Tuesday 24 July 2012
The Risks of Mountain Bike Riding
In a microcosm study of mountain bike injuries Zachary Ashwell, a fourth year medical student who has a background in engineering, took statistics of injuries suffered by individuals who rode mountain bikes. An avid biker himself he knows the hazards and pitfalls that a rider can experience especially at Whistler Mountain Bike Park in Canada.
He studied some 898 case reports from the Whistler Health Care Centre 2009 mountain bike season. The specific cases occurred between May 16 and Oct. 12 of 2009.
He found that the typical injury was a 26-year-old male who suffered the injury between 1 and 4 p.m.
Ashwell discovered that 86 per cent of the patients were male, that August is the worst month for injuries, that 12 per cent of the injuries suffered were considered potentially threatening to life, limb or function, and that more than 75 per cent of the bones broken in the bike park were upper body bones.The most severe injuries involved internal bleeding or internal organ injury, spinal cord injury or traumatic brain injury.
Obviously the idea is to have as much safety gear as possible worn by the rider. Of 24 cases where safety equipment was noted only one was documented as not wearing armor. The other 23 were documented as wearing a variety of protective devices beyond a helmet, including knee and elbow pads, full body protective suits and neck guards. At the risk of divulging a possible business idea this writer suggests that someone should invent a kind of ”airbag garment” to protect the mountain bike rider when he falls.
As stated above one of the more severe injuries that can occur to bike riders when they fall is Spinal Cord Injury (SCI) or Traumatic Brain Injury (TBI).
When that occurs and the initial emergency treatment has passed the patient will need the best physical therapy solution to cope with any limb movement disability issue he has. The TUTOR system is in the forefront of such physical therapy products and has been developed to assist patients to get the most intensive exercises so that the limb can return to its former mobility stage (and the patient can again ride his bike??)
The devices (HANDTUTOR, ARMTUTOR, LEGTUTOR, 3DTUTOR) are sophisticated, ergonomic and comfortable gloves and braces and have become a key system in neuromuscular rehabilitation and physical therapy for interactive rehabilitation exercise. The TUTORs are connected to exclusive software that implement an impairment based program with augmented feedback and encourage motor learning through intensive active exercises. The physical therapist records and evaluates the progress made by the patient and designs a customized exercise program for that patient. The TUTOR system, fully certified by the FDA and CE is now part of the rehabilitation program of leading U.S. and foreign hospitals and can be used in clinics in their home through the use of tele-rehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Monday 23 July 2012
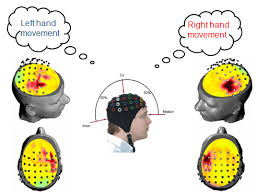
Improving Brain Function After Stroke
Dr. Robert Rennaker and Dr. Michael Kilgard of the University of Texas, Dallas recently proved how nerve stimulation when paired with specific experiences, like movements or sounds, is able to reorganize the brain and even improve its function.
What they discovered could lead to new treatments for stroke, autism, tinnitus, and other disorders.
The researchers looked at whether by repeatedly pairing vagus nerve stimulation with a specific movement it would change neural activity in laboratory rats’ primary motor cortex. They paired the vagus nerve stimulation with movements of the front limbs in two groups of rats.
After a period of five days of this stimulation and movement pairing, the researchers examined the brain activity of the rats. Those who received the training together with the stimulation displayed large changes in the organization of the brain’s control system. Those animals receiving identical motor training without stimulation pairing didn’t exhibit any brain changes, known as plasticity.
Patients suffering from strokes or other brain trauma often have rehabilitation that includes repeated movement of the affected limb in order to regain motor skills. It is surmised that repeated use of the affected limb will cause reorganization of the brain which is essential to recovery.
Dr. Rennaker stated that there was a suggestion from the research that pairing vagus nerve stimulation with standard therapy could result in a more rapid and extensive brain reorganization. This would offer the potential for speeding recovery following a stroke.
He further stated “Our studies in sensory and motor cortex suggest that the technique has the potential to enhance treatments for neurological conditions ranging from chronic pain to motor disorders. Future studies will investigate its effectiveness in treating cognitive impairments”.
Vagus nerve stimulation has an excellent safety record in human patients that suffer from epilepsy. Therefore the technique researched provides a new method to treat brain conditions such as dyslexia and schizophrenia.
Future human patients may have access to more efficient therapies that are minimally invasive and avoid long-term use of drugs if the studies are confirmed.
To provide repeated movement of a stroke affected limb the TUTOR system has been in the forefront of physical therapy products. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been developed to provide intensive and active movement of disabled legs, hands, wrists, elbows and other upper and lower limbs. The ergonomic gloves and braces that make up the TUTOR system are connected to dedicated software that allows the therapist to fully customize the exercises to the patient’s movement ability. In addition the therapist can objectively and quantitatively evaluate and report on the treatment progress. The TUTOR rehabilitation system optimizes the patient’s motor, sensory and cognitive performance and allows him to better perform everyday functional tasks to improve their quality of life.
The TUTOR system is currently in use in leading U.S. and European hospital and clinics. They are fully certified by the FDA and CE and can be used at the patient’s home via telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Sunday 22 July 2012
Can Prayer Help Prevent Stroke?
Do you want to prevent having a stroke? One of the most important methods is to eliminate any risky practices you may have. Of course there are certain things we can’t change such as: genes, age and gender but we can change diet and physical activity.
Adopting a diet which is low in salt and fat but high in fiber is a beginning. Vitamin B rich foods such as spinach, broccoli, carrots, salmon, herring, chicken, walnuts, almonds, sunflower seeds and whole wheat would be helpful. It is known that Vitamin B foods lower homocysteine levels and too much of this amino acid in the blood increases the risk for stroke. There are other foods that lower the risk of stroke and they include cinnamon, garlic, olive oil, onion, dark chocolates, green tea, oatmeal and strawberries.
People that have diabetes should take necessary steps to prevent stroke as well. Diabetics are at risk and therefore should manage their diabetes by eating healthy and monitoring their blood pressure.
Exercise is is a crucial element in stroke prevention as obesity is a stroke risk. Exercise will help take off pounds and maintain healthy weight. Cholesterol levels should be checked regularly.
The state of one’s mental health can also increase stroke risk. Stress can be very damaging, if left unmanaged. It raises blood pressure, which makes the heart pump harder. One of the ways to reduce stress is with physical activity such as exercise or deep breathing. Reading and prayer or meditation can also relieve stress.
Preventing high blood pressure is crucial to stroke prevention. That can be done by avoiding, or at least reducing, the consumption of high-fat foods such as: butter, red meat, eggs, shortening, certain cheeses and dairy products. Reducing the amount of salt is advisable. Sugar, caffeine and alcohol can raise blood pressure, which is a risk factor of stroke.
Here are some common symptoms of stroke which, if experienced, should be brought to the attention of medical experts immediately. Sudden weakness or numbness in the face or limbs; slurred speech or drooling; numbness on one side of the body; problems with balance or walking; dizziness; confusion; or a severe headache.
Unfortunately, even with the best prevention, stroke can still occur and one of the after effects can be the paralysis of a limb. When that occurs and after the patient is stabilized the emphasis will be to rehabilitate the leg or arm that is affected. Fortunately, today there are some very good physical therapy solutions such as the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR.
The TUTOR system has become key in neuromuscular rehabilitation for stroke victims and those recovering from brain and spinal injuries, Parkinson’s, MS, CP and other limb movement limitations. These innovative devices implement an impairment based program with augmented motion feedback that encourages motor learning through intensive active exercises and movement practice. They consist of a wearable glove or braces that detect limb movement showing the patient how much active or assisted active movement he is actually doing. The rehabilitation software uses special games to set a new target for this movement in terms of the patient’s ability to move their limb. The devices then measure the limb movement and give feedback to the patient in trying to gain this new movement objective. Consequently the patient understands which effort is more successful in getting him to move their affected limb again. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are now part of the rehabilitation program of leading U.S. German, Italian, French, UK and other foreign hospitals. They are adaptable for children as well as adults and are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.

Wednesday 18 July 2012
What (Not) to Eat After a Spinal Cord Injury
What does food have to do with spinal cord injury one might ask. However after such an injury, a person’s metabolism can often change quite a bit. Since fewer muscles are being used, people with a spinal cord injury don’t need as many calories per day as before the injury. So, if their eating habits do not change , they may be at risk for obesity and other negative health conditions. It is necessary to avoid certain types of food after a spinal cord injury in order to help a person maintain a healthy weight.
Fast foods are high on the list of what to avoid after a spinal cord injury, or SCI, as they tend to put too many calories into each meal. Eating 1200 calories in one meal, as fast foods generally contain, may be half the person’s daily intake The National Guideline Clearinghouse, states that a person with a spinal cord injury requires around 10 percent fewer calories per day than the average person. If they are severely impaired or inactive they may need even less. Avoiding the excess fat
and cholesterol that these foods tend to contain is necessary.
According to The Spinal Cord Injury Network people with paraplegia or quadriplegia should also limit their sodium intake to no more than 500 to 1,000 mg daily. Taking more than that may cause excess fluid retention, which can make their bodies more susceptible to negative health conditions. Too much sodium can raise blood pressure,which is a risk factor for heart disease and stroke. Sodium is prevalent not only in salt but also in many sauces, condiments and pre-packaged meals. It is important to read labels of such foods before ingesting them.
Just like salt, SCI patients should also avoid too much sugar as they are high in calories and give no nutrition. According to The Baylor College of Medicine such foods should make up only a small part of the daily diet for those living with SCI. Included in these foods are sodas, candy, cookies and cakes. Sweetened beverages, such as juices or tea mixes, may also contain too much sugar. Likewise alcohol consumption should be limited to one drink per day for women with SCI and two for men as a maximum.
Other foods for SCI patients to avoid would be chips, fried chicken, certain oils, butter and fatty meats.
So much for food intake for the SCI patient but in order to strengthen the limbs and muscles of these patients the proper exercises have to take place. One of the most cost effective physical therapy solutions can be found today in the TUTOR system. It consists of motivating and challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. Controlled exercise practice will help to prevent the development of compensatory movement patterns. The dedicated software allows the therapist to fully customize the exercises to the patient’s movement ability. In addition the therapist can objectively and quantitatively evaluate and report on the treatment progress. The rehabilitation system optimizes the patient’s motor, sensory and cognitive performance and allows the patient to better perform everyday functional tasks to improve their quality of life.
The TUTOR system (HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR) are available for children as well as adults and are fully certified by the FDA and CE. Currently in use in leading U.S. and European hospitals the TUTORs can be used in the patient’s home through telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Tuesday 17 July 2012
Prehabilitation–a Definition
PREVENTION & REHABILITATION: Two words that are not usually mentioned in the same breath. They actually are at opposite ends of the spectrum. However they really can go together because as much as rehabilitation serves to heal the injured, prevention or ”prehabilitation” can prevent the injury.
To explain it further there are two areas of rehabilitation:
a) Prehabilitation: which is exercise therapy undertaken by athletes and others to try to reduce the risk of injury.
b) Rehabilitation: is exercise therapy which is used to strengthen muscles around limbs and thereby attempt to return the use of an affected limb to its previous healthy state and also to prevent the injury from recurring. This method can be used to build up muscles and reduce injury around the shoulder, arm, leg and other upper and lower limbs of the body. Players of contact sports such as Rugby in the UK or football in the U.S., as an example, can be the beneficiaries of such prehabilitation.
Using the best physical therapy solutions for prehabilitation would add to the success of prevention of severe injuries. Such physical therapy products as the TUTOR system will afford the athlete and others to accomplish the goal of muscle toning and strengthening. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been introduced to provide intensive exercises for disabilities arising from stroke, CP, MS, brain/spinal cord injuries and other upper and lower limb injuries or diseases. The same TUTOR system can be used to exercise various muscles of the body on a regular basis to help prevent injury due to sports and other accidents. The TUTORs are ergonomically designed gloves and braces that are attached to various parts of the body and through powerful evaluation software accessed by sensors in the braces that allow the patient to perform intensive exercises. The exercises are monitored by physical therapists who then design a custom made program appropriate for that patient’s ability level.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are fully certified by the FDA and CE. They are available for children as well as adults and can be used in the patient’s home through telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Monday 16 July 2012
How Much Salt to Add to Your Food
As published on Wednesday, April 25, 2012 in the journal STROKE, Dr. Francesco P. Cappuccio, of the University of Warwick in the UK stated that older adults with salty diets may have an increased risk of suffering a stroke.
The results were in a study of 2,700 older, mostly minority adults. They got well above the recommended sodium intake and were nearly three times as likely to suffer a stroke over 10 years as people who met guidelines recommended by the American Heart Association (AHA).
As people’s sodium intake goes up, their blood pressure will likely increase as well.
What is not as clear, though, is whether a salty diet may mean higher risks of heart attack and stroke later on.
Unlike blood pressure, which can change quickly, stroke and heart disease are more long-range complications. So a study of the relationship between people’s sodium intake and their risk of heart problems and stroke is more difficult.
At this time, the AHA suggests that people not consume more than 1,500 milligrams a day. The World Health Organization advises a limit of 2,000 milligrams.
The people in this study — mainly black and Hispanic New Yorkers — consumed 3,031 milligrams of sodium per day.
The findings are based on 2,657 adults who were interviewed about their health and lifestyle and then completed dietary questionnaires. They were 69 years old, on average, when the study began.
During the next 10 years, there were 235 strokes in the group. Those that downed 4,000 or more milligrams of sodium each day were almost three times more likely to suffer a stroke as those who kept their daily sodium below 1,500 milligrams.
Among the 558 people consumed more than 4,000 milligrams per day, there were 66 strokes.
That compared with 24 strokes among the 320 people who kept within the AHA guideline.
Hannah Gardener, a researcher at the University of Miami School of Medicine who led the study said “We can’t definitively draw conclusions about cause-and-effect .
There can be a number of other factors to take into consideration in addition to salt intake. As an example
smoking habits, exercise levels, education and health conditions like diabetes and high blood pressure need to be taken in to consideration.
Although few Americans adhere to the AHA guidelines they should be followed according to Gardener.
Interestingly, it’s estimated that the typical U.S. man takes in 4,000 milligrams of sodium a day, while women typically ingest 2,800 milligrams.
Salt is pervasive in the food supply — from canned soups and sauces, to breads and cereals, to processed meats — and it can be challenging to cut down. Americans receive almost 80 percent of their sodium from prepared foods on supermarket shelves and in restaurants, rather than at home.
Gardener further states that it is important to read product labels to know beforehand how much sodium there is in the product.
Eating fruits, vegetables and whole grains, as much as possible will also alleviate the problem.
The researchers suggest that responsibility should also rest on government regulations and the food industry.
In England, the government has begun to regulate the processed food industry. New York City has instituted the National Salt Reduction Initiative. This move tries to coordinate local and state governments and health groups to work with the food industry to cut sodium in packaged foods and restaurants.
Heinz, Kraft Foods and Starbucks, have already signed on to meet salt targets.
Unfortunately, at this time and age people still take in too much sodium so strokes will still occur. When they do and the initial medical treatment is completed it behooves doctors and other medical staff and facilities to supply the best physical therapy solutions available to treat any paralysis that may exist as a result of the stroke. Such physical therapy products are the TUTOR system.
Rehabilitation using the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR is instituted in the USA at major in-patient and out-patient clinics as well as at private physical therapy clinics. Many patients including stroke victims can also avail themselves of the TUTOR system through the use of tele rehabilitation when they are at home or in a location far from a qualified rehabilitation center. The TUTOR products have been developed to allow for functional rehabilitation of the whole body including the upper and lower extremity. The system consists of ergonomic wearable devices and dedicated rehabilitation software that provide patient instructions and feedback to encourage intensive controlled exercise practice. The TUTOR system exercises multijoints within the normal movement pattern which prevents the development of undesired and compensatory joint movement. It therefore ensures better performance of functional tasks. This is important in stroke, brain, spinal cord (SCI) and Cerebral Palsy rehabilitation in addition to other neurological and orthopedic injury and disease. Additional features of the TUTOR system include quantitative evaluation and objective follow up that is important in the physiotherapists treatment of the stroke patient. The TUTORS are FDA and CE certified and are available for children as well as adults. See WWW.MEDITOUCH.CO.IL for more imformation.
Sunday 15 July 2012
What to Expect From Stroke Rehabilitation.
Dr. Komaroff is a physician and professor at Harvard Medical School and gives the following advice
Rehabilitation helps return abilities impaired by a stroke. How much progress one makes and how quickly it occurs will depend on how severe the stroke was and the part of the brain that was affected.
Strokes can affect muscle strength, senses (like pain), one’s ability to speak and to understand speech, vision, emotions, thinking and level of consciousness. Some people only suffer mild unilateral weakness with nothing else wrong. Other people lie in a coma.
New techniques have been learned in recent years that sometimes lead to recovery that at one time were not possible.
Rehabilitation may occur in the hospital, a rehab facility or at home. One or more specialists may be involved. These may include a physiatrist, rehab nurse, physical or occupational therapist, speech-language pathologist or a recreational therapist.
The strategies used will depend on the patient’s goals for therapy. Some common goals include rebuilding strength, relearning to walk, improving speech and recovering memory. On the other hand rehab can also help a person adapt to a permanent disability, if necessary.
Physical rehab may include walking up or down stairs, walking on a treadmill and using hand or leg weights. Even if the patient can’t bear weight on his legs exercise may still be possible. This may have to be done while partially supported by a harness. Many patients exercise in a swimming pool, where water can support some of the weight.
The therapist may also stimulate natural movements in the arms and legs. This can help restore neurological pathways at the same time as it strengthens muscles and improves circulation.
Regaining skills for regular everyday living is another important goal. The patient will learn practical techniques to make washing, dressing, driving and other routine activities more manageable.
The therapist may teach speech and language skills and may include exercises to improve comprehension, speaking, reading and writing. It may also help restore the ability to swallow safely which is often impaired by a stroke.
Then there is cognitive rehab that teaches strategies to compensate for problems with learning, memory, and awareness.
Rehab usually takes time and hard work. patients sometimes get discouraged but rehab can make the crucial difference between regaining previous ability to function or remaining impaired.
Some patients make little progress after a month of work, every day, with rehabilitation therapy. Then, they suddenly seem to make considerable progress. They should not give up. Stroke rehab really can make a difference.
Finding and using the best physical therapy solutions often includes products like the TUTOR system. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been developed to assist in exercising stroke affected limbs.
The TUTORs have become a key system in neuromuscular rehabilitation and physical therapy for interactive rehabilitation exercise. These innovative devices implement an impairment based program with augmented feedback and encourage motor learning through intensive active exercises. These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. The training is customized by the occupational and physical therapist to ensure that the patient stays motivated to do intensive repetitive manual therapy and exercise practice. The TUTORs are now part of the rehabilitation program of leading U.S. and European hospitals with the TUTORs being used in clinics and in the patient’s home. Home care patients can be supported by the occupational and physical therapist offering tele-rehabilitation. The TUTORs are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.

Thursday 12 July 2012
Why Patients Don’t Always Cooperate With Physical Therapy
A study was conducted to determine why patients don’t always cooperate with physical therapy. The question was, whether the patient was non compliant because of the patient’s personal characteristics or illness or because of the patient’s attitude or to the physical therapist‘s behavior.
A questionaire was sent to 300 Dutch physical therapists. More than two thirds responded. The results showed that there were 3 main factors to noncompliance on the part of patients to physical therapy. First, and the strongest reason, was the perception of the barriers to the therapy and encountering those perceptions. Second, was the lack of feedback they received and third, the feeling of helplessness they felt. The results also showed that non compliance with physical therapy was because of the characteristics of the illness rather than the illness itself. If the patient received a negative prognosis it would produce more non compliance.
No differences were seen between male and female noncompliance but there was a difference between more or less educated patients with the less educated being more compliant than the highly educated.
The conclusion of the study seems to be that physical therapists should investigate more thoroughly problems that patients encounter with compliance and to seek the solutions to those problems before proceeding so that there can be mutual cooperation between patient and therapist.
A significant part of compliance can be the method(s) used in the physical treatment itself. If the treatment is enjoyable, shows results and is set at at the patient’s level he will tend to be more compliant than if it is just routine and there is no feedback on progress. Such is the goal of the TUTOR program. The TUTORS (HANDTUTOR, ARMTUTOR, LEGTUTOR, 3DTUTOR) are physical therapy products that allow the patient to receive intensive exercises in a fun way–through the use of games created exclusively for the TUTORs. Physical therapists monitor the exercises, record and evaluate the results and then customize a program for that particular patient. This in turn gives the patient satisfaction as he sees steady improvement in rehabilitating his affected limb after a stroke or other medical incident that he experienced.
The TUTORs are fully certified with the FDA and CE and are currently in use in U.S. and European hospitals and clinics. The TUTORs are available for children as well as adults and also at home through the use of telerehabilitation. More information on these cost effective devices can be seen on WWW.MEDITOUCH.CO.IL

Wednesday 11 July 2012
Development Coordination Disorder or Just Plain Clumsiness?
Developmental coordination disorder (DCD) is a childhood disorder that can lead to poor coordination and clumsiness.
Approximately 6% of school-age children have some kind of developmental coordination disorder. Children with this disorder may:
Have an unsteady walk
Have trouble holding objects
Trip over their own feet
Run into other children
Developmental coordination disorder may occur by itself or together with other learning disorders, such as communication disorders or disorders with written expression.
Appropriate physical education and perceptual motor training are amongst the best ways to treat coordination disorder. The use of a computer to take notes may help children who have trouble with their writing.
It is also known that children with developmental coordination disorder are three times as likely to be overweight than other children their age. It is vital to encourage physical activity in order to prevent obesity.
How well a child does depends on how severe the disorder is. Though the disorder does not worsen over time, it usually continues into adulthood.
There are sometimes complications from DCD such as:
Low self-esteem resulting from poor ability at sports and teasing by other children
Learning problems
Weight gain because of a lack of physical activities (such as sports)
Repeated injuries
An appointment with a health care provider is vital to check the child’s development.
One of the most cost effective and fun ways to treat DCD may be by using the HANDTUTOR, ARMTUTOR or LEGTUTOR. These recently developed physical therapy products are available for children as well as for adults and are used for treating a variety of disorders and post surgery movement issues. The child who has a coordination problem will enjoy being involved in the many games that the TUTOR system has to offer. These exclusive exercise programs that were designed specifically for various limb movement disabilities can also provide just the right amount of movement that children with DCD need.
The TUTOR system is fully certified by the FDA and CE and can be used at home through the use of telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Tuesday 10 July 2012
Acquired Brain Injury–What is it and What Can Be Done?
Many people suffer from brain injury which usually is caused by a traumatic event such as an accident or fall. However there is also what is called Acquired Brain Injury which can be a result of a stroke, tumor or infectious disease.
It was announced on July 10 that in London a campaign has begun by the United Kingdom Brain Injury Forum (UKBIF) that will highlight the need for easier and earlier access to rehabilitation for ABI patients. The aim of the campaign is to improve existing services and to do more for these unfortunate individuals.
It is known that the effects of ABI include physical, emotional, sensory and cognitive problems. Also that the effects can be temporary, permanent, light or severe. Sometimes the disabilities are not obvious. Results may include relationship breakdowns, loss of employment and change of personality.
In the UK alone approximately 150,000 people per year have some kind of brain injury and the costs for ABI care was more than 1 billion pounds Sterling just in hospital costs in 2007. Community care and rehabilitation cost another 4 billion pounds. One factor that is known about brain injury is that early rehabilitation may help to reduce length of hospital stays. Because of these facts it is important that all costs for future care are available and that the highest standard of care and rehabilitation be administered.
One of the latest physical therapy solutions is the TUTOR system. It is very cost effective and therefore can keep the costs of rehabilitation down while affording the patient the best of care. The TUTORs which include the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are ergonomically designed gloves and braces that are strategically placed on the affected part of the body and then through exclusive software the patient can exercise his affected limb. Physical and occupational therapists monitor this activity and record and evaluate the patient’s progress and then design a custom made exercise program for the patient at his ability level. The TUTORs are available for adults as well as children, are fully certified by the FDA and CE and can be used at home through the use of telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Monday 9 July 2012
Action Observation Treatment (AOB) as a Means of Physical Rehabilitation
AOB may be defined as when the observation of actions performed by others activate in an observer the same neural structures as when he/she actually performs the same actions.
There is evidence that the observation of actions activates the same cortical motor areas that are involved in the actual performance of the observed actions. The neural substrate for this is the mirror neuron system. We capture this neuronal system and then re-enact the stored motor representations as a means for rehabilitating motor control. This may be called motor imagery.
In a study employing AOB eight stroke patients with moderate, chronic motor deficit of the upper limb participated. A significant improvement of motor functions during a 4-week treatment, as compared to the stable pre-treatment baseline, and compared with a control group was found. The improvement lasted for 8 weeks after the end of the intervention.
Physical rehabilitation, for a large part may be seen as a learning process where old skills have to be re-acquired and new ones have to be learned on the basis of practice. Active exercising creates a flow of sensory information. It is known that motor recovery and motor learning have many aspects in common. Both are largely based on response-produced sensory information. Numerous studies have indicated that motor imagery may result in the same plastic changes in the motor system as actual physical practice. Motor imagery is the mental execution of a movement without any overt movement or without any peripheral (muscle) activation. It has been shown that motor imagery leads to the activation of the same brain areas as actual movement. Therefore motor imagery may play an important role in neurological rehabilitation. Furthermore, the observation of a movement may play a similar role in learning movement. The use of motor imagery in neurological rehabilitation may have a value even if it’s on theoretical grounds and on the basis of the results of studies with healthy subjects.
For actual physical therapy solutions for stroke patient rehabilitation the TUTOR system is one of the most effective products available. The TUTOR system, consisting of the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR, are ergonomic gloves and braces with speed and position sensors that are placed on affected parts of the body. Specialized powerful software is used to allow the patient to exercise his affected limb. The information is then recorded and evaluated by the physical therapist who then designs a customized exercise plan for that patient. The TUTORs are currently in use in leading U.S. and European hospitals and clinics and are fully certified by the FDA and CE. The patient can avail himself of the TUTOR system at home through the use of telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.
Sunday 8 July 2012
Dolphin Assisted Therapy (DAT) and Cerebral Palsy
Dolphins have been used to treat a variety of ailments including autism, cerebral palsy, trauma and cancer among other disabilities.
Dolphin-assisted therapy (DAT), as a part of animal-assisted therapy and complementary and alternative medicine, yields several positive results. A study in the Ukraine called ”Dolphin Swim” used 37 participants who were parents of special needs children. The children suffered from a variety of diagnoses which included emotional and physical disorders. Five treatment programs took place over a span of 2 weeks. A comparison was made with pretreatment and post treatment using DAT (Dolphin Assisted Therapy). The results showed positive behavioral changes in the affected children.
In Israel at the Eilat Dolphin Reef Dr. Ilan Kutz of the Meir Medical Center has supervised the unusual treatment and rehabilitation of trauma victims. DAT is not a cure but alleviates symptoms significantly. Dolphins are very intelligent creatures and have a language of clicks and physical movements. They enjoy communicating with humans and like to be touched, petted and cuddled. The mammals react to the person if they feel a connection to him and then they will give unconditional love. In a particular case of a young man that was severely beaten and even after his physical wounds were healed he didn’t speak. Working with the Dolphins greatly improved his swimming skills and he now speaks normally.
Aside from this unusual therapy the CP patient can hope to improve limb movement ability with the use of the TUTOR system. This most cost effective physical therapy solution (as is the dolphin therapy) is currently used in leading U.S. and European hospitals and clinics. The system which includes the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR are ergonomic wearable devices together with powerful dedicated rehabilitation software. The TUTOR system consists of motivating and challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. The physical therapist can then record and design a custom made exercise program for that particular patient’s needs.
The Tutors are also available for adults and children and can be used in the patient’s home through the use of telerehabilitation. They are fully certified by the FDA and CE.
See WWW.MEDITOUCH.CO.IL for more information.

Friday 6 July 2012
Alcopop–what is it and what does it do?
A not so new but dangerous trend has begun appearing that affects teenagers around the world. ALCOPOP is an alcoholic drink that tastes like a soft drink. The sweetness masks the alcohol. Also known as ”girlie drinks”, clear malts, flavored malts and ”cheerleader beer”, alcopops are used by more girls than boys. Children as low as 13 and sometimes lower are exposed to it. Teenagers in the ever longing quest to become an adult as fast as possible love to imbibe when they are in social gatherings and family events. Drink advertisers disseminate their products on TV before 9 p.m. when there is a large teenage audience. Alcopops are a soft entry to the hard world of alcohol.
The ramifications are enormous. Statistics have shown that a meaningful percentage of teens get into risky situations following the drinking. Aside from the fact that they become educated into the world of alcoholism they also run into trouble at a young age when they get into cars and begin driving under the influence of liquor. Even if they don’t drive they accompany friends who drive after having had several alcoholic beverages. The risk of accidents and unwanted sexual activity increases in proportion to the amount they drink. If there is no parental or other supervision the child will continue with this habit into adulthood. Just one of the long term results of this phenomenon is brain impairment. It also can cause liver disease, cardiac problems and, of course, alcoholism with all its ramifications.
If, unfortunately, a brain injury occurs then after the initial treatment is over and rehabilitation begins one of the best physical therapy products available today is the TUTOR system.
The recently developed HANDTUTOR and its sister devices (ARMTUTOR, LEGTUTOR, 3DTUTOR) have become a key system in neuromuscular rehabilitation for brain and spinal injuries and other limb movement limitations. These innovative devices implement an impairment based program with augmented motion feedback that encourages motor learning through intensive active exercises and movement practice. The HANDTUTOR, ARMTUTOR, LEGTUTOR, 3DTUTOR consist of wearable glove and braces that detect limb movement showing the patient how much active or assisted active movement he is actually doing. The rehabilitation software uses special rehabilitation games to set a new target for this movement in terms of the patient’s ability to move his limb. The devices then measure the limb movement and give feedback on the success of the patient for this new movement objective. In this way the TUTOR system provides exercises that are challenging and motivating and allows for repetitive and intensive exercise practice. The TUTOR system is now part of the rehabilitation program of leading U.S. German, Italian, French, UK and other foreign hospitals. Exercises can be done from the patient’s home through the use of telerehabilitation. The devices are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.
Wednesday 4 July 2012
Don’t Underestimate Pre Knee/Hip Surgery Exercises
All those that undergo knee or hip replacement surgery need to get into anexercise program following surgery. However it is equally important to have an exercise program prior to these surgeries as well so as to strengthen the muscles around the joint. This will both enhance the recovery and properly support the new joint. How much exercise to do is an individual choice and will depend on a number of factors. If the exercise causes pain it would be better to curtail it. It is preferable to exercise once or twice a day every day before surgery and to do five repetitions of each exercise and then gradually increase them until the actual date of surgery. Doing the exercises in bed lying down is excellent. Your doctor or physical therapist can prescribe specific exercises for your condition.
An excellent plan would be to use the LEGTUTOR as a physical therapy product as it has a reputation for ease and comfort. The LEGTUTOR consists of a safe and comfortable leg brace with position and speed sensors that precisely record 3 dimensional hip and knee movements. The LEGTUTOR has a range of motion limiter that can limit the dynamic range of knee extension and flexion. Rehabilitation games allow the patient to exercise Range of Motion (ROM), speed and accuracy of movement. The LEGTUTOR facilitates evaluation and treatment of the lower extremity including isolated and combined hip and knee movements. The LEGTUTOR together with its sister devices (HANDTUTOR, ARMTUTOR and 3DTUTOR) are currently used successfully in leading U.S. and European hospitals for a variety of disabilities including stroke, CP, MS Brain and Spinal cord injury and others affecting the upper or lower limbs. The TUTOR sytem is available for children as well as adults and are fully certified by the FDA and CE. The TUTORs can also be used at home through telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Tuesday 3 July 2012
Obesity–When Will It End?
The information below is not necessarily new but because of its importance bears repeating.
Obesity is a worldwide problem and in some cases is more serious than malnutrition. A change of lifestyle and eating the wrong foods contribute to being overweight.
The problem exists in both developed and developing nations and has grown to be a global epidemic. The figures have reached one billion with about 300 million classified as clinically obese.
There are more than one billion overweight adults in the world, and at least 300 million of them are clinically obese. One of the problems is that very little is known about what causes obesity. In addition information about consequences and remedies is also somewhat lacking .
What is known is that the U.S. has the highest number of obese people followed by Mexico, the UK and Australia.
The lowest percentages are in Japan and Korea. There has been tremendous growth of obesity during the 1990s in the U.S. and experts feel that it will increase further. The problem, sadly, also affects children. Multiple studies have shown that obese children are likely to become obese adults.
The problem is not only one of health but also economic. Studies have shown that obese people have lower employment rates. Medical problems cause health costs to rise. These are costs related to obesity causing many diseases such as cancer, stroke, diabetes, heart disease and even depression.
Obesity is caused by the difference between calorie intake and usage. There is a difference of opinion as to what is a greater cause. Some argue that the growth of fast food outlets is a major cause. Others feel that it may be due to snacking between meals. Still others feel that the cause may be lack of exercise. Following an evolutionary chain some people feel that the cause may be the increased rate of industrialization and the resulting lack of time by workers. This brings about an increase to ”grab some food” from a fast food outlet instead of taking the time to prepare a home cooked meal.
Some research has shown that Hispanics and black people have a higher incidence of obesity than wealthier and more educated people have. All in all this shows that the problem is complex and it would be difficult to pinpoint a particular reason for obesity.
There are more statistics available and there is a myriad of advice as to how to counteract the problem. Those that are interested can certainly avail themselves of this information.
As stated, one of the direct results of obesity is the increased possibility of getting a stroke. This debilitating disease usually results in at least a partial paralysis of an arm or leg or both. When that occurs and the initial medical attention is completed a system of physical rehabilitation is instituted to try to return full use of the limb to a pre stroke status. When that occurs it behooves the patient to be able to make use of the most efficient physical therapy solutions. Such a solution is the TUTOR system. Consisting of the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR these devices afford the patient a state of the art exercise program. The TUTORs are comfortable and ergonomically designed gloves and braces that are placed startegically on the affected limb. The dedicated and exclusive software that is used consists of specially designed games that allow the patient to maximize his own efforts (rather than a robot’s efforts). The physical and occupational therapists assigned to that patient can tailor make a specific exercise program that is designed for that particular patient.
The TUTORs are currently in successful use in leading U.S. and European hospitals and clinics. They are fully certified by the FDA and CE and are available for children as well as adults. In addition they can be used in the patient’s home through the use of telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Monday 2 July 2012
Bi Lateral Stroke Rehabilitation
Even though strokes typically affect only one side of the body, rehabilitation appears to work best when both sides of the body are engaged in it. A study done by Ken Takitama of the University of Tokyo and Masato Okada of the RIKEN Brain Science Institute in Wako, Japan, and published on June 27, 2012, found that the two-sided approach was especially important in getting functioning back in a weakened arm and hand. Recovery of movement in the upper limb usually takes longer than that of the leg and foot.
The researchers wrote that their study suggests that “bimanual movement facilitates the reorganization of a damaged motor cortex because this movement induces rotations in the preferred directions (PDs) of motor cortex neurons . . . Although previous computational studies investigated the unimanual movements of stroke patients, individuals often move their arms bimanually. Bimanual movement is effective for the recovery of partially paralyzed arm movement . . . Rotations of the encoding PDs facilitate cortical reorganization.”
It is also important to note that several other studies have shown that, as with any motor skill, practice makes perfect when it comes to stroke rehabilitation. Patients that are more serious with repeating therapeutic movements tend to recover faster than those who are more lax in their exercising.
Taking advantage of the most efficient physical therapy solutions is vital to progress for unilateral or bilateral stroke rehabilitation. The HANDTUTOR, ARMTUTOR for upper limb and the LEGTUTOR for lower limb paresis are physical therapy products that can speed up the rejuvenation of disabled limbs due to stroke.
The TUTORs consist of motivating and challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. Controlled exercise practice will help to prevent the development of compensatory movement patterns. The dedicated software allows the therapist to fuly customize the exercises to the patient’s movement ability. In addition the therapist can objectively and quantitavely evaluate and report on the treatment progress.The rehabilitation system optimizes the patient’s motor, sensory and cognitive performance and allows the patient to better perform everyday functional tasks to improve their quality of life.
Currently in use in leading U.S. and European hospitals and clinics the very cost effective TUTORs are available for adults as well as children and are fully certified by the FDA and CE. They can be used in the patient’s home via telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Subscribe to:
Posts (Atom)