Simon Martin reporting in YORK REGION.COM on September 17, 2011 relates the following story.
Life was going according to plan for Dana and Jared Florence in 2008.
They had good careers and it was a natural step to add a child to the mix. So it was a bit shocking when Ms Florence found out she was having triplets. It was even more earth shaking when they were born 15 weeks premature.
The Florences’ lives had been turned upside down.
In the beginning, it was 50-per-cent chance of survival, Ms Florence said.
“The first few months, it was day by day.”
The triplets — Taylor, Cole and Brody — were discharged from hospital at different times. It was only after six months in intensive care that the babies were all home with their parents.
“It was a difficult time,” she said. “All the things I thought I would experience were different. I would have to wash my hands before touching my own baby.”
Once at home, it became clear the triplets weren’t developing at the rate expected of them. At 10 months, all three was diagnosed with cerebral palsy — a brain condition with no known cure.
But their challenges fuelled the couple’s desire to do something to make a difference for children such as their own.
“We were looking for more in terms of what was happening with research,” she said.
They created Three To Be to help support child neurological disorders research and the response has been fantastic, Ms Florence said.
The organization hosted its second annual Stems of Hope Gala Saturday at Toronto’s Kool Haus and is optimistic it surpassed last year’s total.
Last year, the gala raised more than $500,000, with proceeds going to stem cell research at Toronto’s Hospital for Sick Children and programs at Holland Bloorview Kids Rehabilitation Hospital.
This year, the group raised enough to purchase the Paediatric Lokomat Pro for Holland Bloorview, which is piece of equipment that has the potential to help teach children to walk.
The Barenaked Ladies, Alex Bilodeau and Alexander Richards were just some of the celebrities on hand.
“[Three To Be] has become so much bigger than we could have ever imagined,” Ms Florence said.
Ms Florence grew up in Thornhill and was part of the first graduating class from Westmount Collegiate Institute. The community has really gotten behind the cause, she said, noting her parents still live in Thornhill.
Ms Florence, who now lives in Toronto, said her children mean the world to her.
“It has been such a journey. They are the most beautiful, smart, inspiring people I have ever met,” she said.
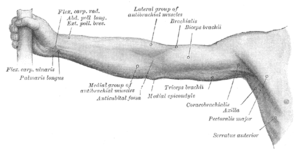
The HandTutor, ArmTutor and LegTutor have been instrumental in augmenting functional movement for patients suffering from Cerebral Palsy and other debilitating diseases that affect the joints. Children such as the Florences can enjoy the various games programmed into the dedicated software.
The system consists of motivating and challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. Controlled exercise practice will help to prevent the development of compensatory movement patterns. The dedicated software allows the therapist to fully customize the exercises to the patient’s movement ability. In addition the therapist can objectively and quantitatively evaluate and report on the treatment progress. The rehabilitation system optimizes the patient’s motor, sensory and cognitive performance and allows the patient to better perform everyday functional tasks to improve their quality of life. The Tutor system is FDA and CE certified.