
Friday, 31 August 2012
Ballet: An Art Form or Cause for Rehabilitation
Most of us don’t associate the art of Ballet dance with injury and rehabilitation however ballet is a source of both. There are many causes for such injuries. There may be environmental factors such as faulty dance surfaces. There may be inappropriately fitting footwear leading to foot conditions. There may be spinal cord issues which can be the cause FOR injury as well as a result OF an injury. An incorrect ”turnout” ( the ability of the dancer to turn his or her feet and legs out from the hip joints to a 90-degree position) on the part of the dancer may cause an injury. There may be an inbalance of soft tissue or inadequate quadricep strength. The beautiful but potentially harmful ballet steps of ”plies”-which is a smooth continuous bending of the knees; ”pointe” where the dancer performs steps while on the tips of the toes using a special block shoe and ”demipointe” can all cause serious injury or worse.
Both male and female ballet dancers are susceptible to these injuries so when they occur the very best physical therapy solutions need to be at hand during their rehabilitation. Physical and occupational therapists have been using the TUTOR system to rehabilitate injured limbs of patients suffering from strokes, brain/spinal cord and upper and lower limb surgeries, Parkinson’s disease, Cerebral Palsy, Multiple Sclerosis and many other limb disabling medical conditions. It is only natural that the HANDTUTOR, LEGTUTOR and ARMTUTOR would be used in the treatment of ballet injuries as well.
The TUTORs are comfortable, ergonomically designed gloves and braces that are strategically placed on the affected part of the body and with sensors attached to dedicated software the patient is subjected to intensive exercises. The therapists evaluate the results and then design a personalized exercise program for that patient. These physical therapy products are currently in use in leading rehabilitation hospitals in the U.S. and Europe. The TUTOR system is fully certified by the FDA and CE and can be used by children as young as 5 as well as adults. Telerehabilitation allows the patient to use the TUTORs in his own home.
See WWW.MEDITOUCH.CO.IL for further information.
Wednesday, 29 August 2012
Making the Case for Continuous Physical Rehabilitation for Parkinson’s Disease Patients
In a controlled clinical trial conducted by Comelia L. Cynthia , MD, Glenn T. Stebbins, PhD, Nancy Brown-Toms, BA and
Christopher G. Goetz, MD of the Department of Neurological Sciences, Rush-Presbyterian-St. Luke’s Medical Center, Chicago, IL. an evaluation was made of the effects of physical disability in moderately advanced Parkinson’s patients following 4 weeks of normal physical activity and 4 weeks of a more intensive physical rehabilitation program. They used a timed motor task and a standard assessment of PD severity (the Unified Parkinson’s Disease Rating Scale [UPDRS] with subscales for mentation, activities of daily living [ADL], and motor function. The test was conducted by an investigator who did not know about the physical rehabilitation status of the patient.
Following physical rehabilitation, there was significant improvement in the UPDRS ADL and motor scores, but no change in mentation score. During the 6 months following physical rehabilitation, patients did not regularly exercise, and the UPDRS scores returned to their baseline. The conclusion the researchers reached was that physical disability in moderately advanced PD improves with a regular physical rehabilitation program, but the improvement is not sustained when normal activity is resumed.
Parkinson’s disease patients have a physical therapy solution that has shown to be very effective in restoring movement ability to disabled limbs due to the disease. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3 DTUTOR are physical therapy products that are currently being utilized in leading U.S. and European hospitals and rehabilitation clinics. The TUTORs are gloves and braces that are strategically placed on affected hands, arms, elbows, legs and other joints. The sensors in these devices pick up the patient’s movements through dedicated software. Physical therapists monitor, evaluate and design these movements into a customized program for that specific patient.
Fully certified by the FDA and CE the cost effective TUTORs are available for children as young as 5 and in the patient’s home through the use of telerehabilitation. See WWW.MEDITOUCH.CO.IL for further information.

Tuesday, 28 August 2012
Should a Patient Undergo Rehabilitation After Stroke?
Henrik S. Jørgensen, MD etal of the Department of Radiology, Bispebjerg Hospital, Copenhagen, Denmark cocnducted a study to determine the value of post stroke rehabilitation.
The objective of the study was to evaluate the outcome of stroke divided according to both the severity of the initial stroke and the initial level of disability.
The study took place in a stroke unit of a hospital in Denmark that receives all acute stroke patients admitted from a large catchment area of approximately 240,000 inhabitants within the City of Copenhagen. Under normal circumstances acute treatment as well as rehabilitation is cared for within the stroke unit regardless of age, severity of the stroke and premorbid condition. In this study 1197 patients with acute stroke were used.
The Main Outcome Measures were: Primary outcome was measured as death, discharge to a nursing home, or to the patient’s own home. Secondary outcome was measured as the patient having neurological deficits and/or functional disabilities after rehabilitation was completed and then again 6 months after the stroke occurred. The indices used were the Scandinavian Neurological Stroke Scale and Barthel . The results were as follows: Stroke was initially very severe in 19% of the patients, severe in 14%, moderate in 26%, and mild in 41% of the patients. Two hundred and fifty or 21% of the patients died during their hospital stay, 177 or 15% were discharged to a nursing home, and 770 or 64% of the patients were discharged to their home. After rehabilitation was completed 11% of the survivors still had severe or very severe neurological deficits, 11% had moderate deficits, and 78% had no or only mild deficits; 20% were severely or very severely disabled, 8% were moderately disabled, 26% were mildly disabled, and 46% had no disability in normal daily activities. The conclusions reached were that there is a great need for stroke rehabilitation in the community and the amount of postrehabilitation disability in stroke survivors cannot be exaggerated. Results, though, should not be used as a guideline for selecting patients for rehabilitation in the acute phase as even the most severe cases experience meaningful improvement during rehabilitation.
The question then becomes what is the most effective physical therapy solution that can speed recovery of the affected stroke victim’s limbs. Other than robotic machines which are large and therefore usable only in rehabilitation facilities and hospitals or are cost prohibitive the physical therapy profession has come to know of the effectiveness of the TUTOR system. Consisting of the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR these recently created products are in the forefront of stroke rehabilitation.
These innovative devices implement an impairment based program with augmented motion feedback that encourages motor learning through intensive active exercises and movement practice. The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR consist of wearable glove and braces that detect limb movement showing the patient how much active or assisted active movement they are actually doing. The rehabilitation software uses special rehabilitation games to set a new target for this movement in terms of the patient’s ability to move his limb. The devices then measure the limb movement and give him feedback on his success. In this way the Tutor system provides exercises that are challenging and motivating and allow for repetitive and intensive exercise practice. The TUTOR system is now part of the rehabilitation program of leading U.S. German, Italian, French, UK and other foreign hospitals and can be used at home through telerehabilitation. The TUTORs are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.
Sunday, 26 August 2012
aintaining Strength for Parkinson’s Patients
In an article published in the British Medical Journal, August 23,2012 C.L. Tomlinson et al state that Physiotherapy has only short term benefits in Parkinson’s disease. He further states that there is a wide range of physiotherapy techniques currently in use to treat Parkinson’s disease and that there is little difference in treatment effects. He suggests that there be large, well designed, randomised controlled trials including improved methodology and reporting that are needed to assess the efficacy and cost effectiveness of physiotherapy for the treatment of Parkinson’s disease in the longer term.
The methods used to come to this conclusion were:
A systematic review and analysis of randomised controlled trials.
Literature databases, trial registries, books, and conference proceedings, journals, and reference lists, searched up to January 31, 2012.
Randomised controlled trials that compared physiotherapy with no intervention at all in patients with Parkinson’s disease were used.
Two authors independently collected data from each trial.
Tests for heterogeneity were used.
Outcome measures were gait, falls, functional mobility and balance, clinician rated disability measures, patient rated quality of life, adverse events, compliance, and impairment and economic analysis outcomes.
The results were:
that indirect comparisons of the different physiotherapy interventions found no evidence that the treatment effect was diferent across the interventions for any outcomes assessed, apart from motor subscores on the unified Parkinson’s disease rating scale (in which one trial was found to be the cause of the heterogeneity).
Apparently C.L. Tomlinson isn’t aware of the TUTOR system. These physical therapy products, although not a cure for Parkinson’s, have shown that they can maintain the strength of the patient thereby giving him a longer period of mobility.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have become a key system in neuromuscular rehabilitation for stroke victims and those recovering from brain and spinal injuries, Parkinson’s, MS, CP and other limb movement limitations. These innovative devices implement an impairment based program with augmented motion feedback that encourages motor learning through intensive active exercises and movement practice. The HANDTUTOR, ARMTUTOR, LEGTUTOR, 3DTUTOR consist of wearable gloves and braces that detect limb movement showing the patient how much active or assisted active movement they are actually doing. The rehabilitation software uses special rehabilitation games to set a new target for this movement in terms of the patient’s ability to move their limb. The devices then measure the limb movement and give feedback on the success of the patient in trying to gain this new movement objective. In this way the TUTOR system provides exercises that are challenging and motivating and allow for repetitive and intensive exercise practice. The TUTOR system physical therapy solution is now part of the rehabilitation program of leading U.S. German, Italian, French, UK and other foreign hospitals. As one of the most cost effective PT products on the market the TUTORs can also be used in the patient’s home throughtelerehabilitation. See www.MEDITOUCH.CO.IL for more information.

Monday, 20 August 2012
Fractured Ribs and Physical Rehabilitation
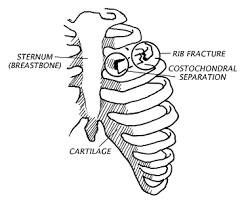
About 300,000 people every year fracture their ribs in the U.S. 72% of these fractures occur in men although postmenopausal women are also prone to them due to osteoporosis. Rib fractures occur as a result of trauma such as falls and sports activities but can also come through severe coughing and even CPR treatment in older adults. A broken or fractured rib may result in internal damage to an organ, tendon or muscle. Severe damage can be done if there is a ‘flail’ chest. That is if 3 or more ribs are fractured in 2 or more places and the ribs are separated from costal cartilege or the sternum.
Earlier treatment included wrapping the chest in bandages or corsets to keep the ribs in place for healing however that is not done now as it limits proper breathing. Improper breathing can cause pneumonia and other problems.
The recommended treatment is rest, gentle exercise, pain medication and targeted physical therapy programs when the pain is less severe. Yoga and other strenuous activities are to be avoided for up to 6 weeks in most cases. Time is the main healer as the ribs heal themselves. It is recommended to take deep breathes and gentle exercises to expand the diaphragm. Sometimes even swimming 45-90 minutes per day can be helpful. Walking and moving helps to keep the airways clear and helps to prevent pneumonia and collapsed lungs.
One of the simple exercises recommended is the ”pendulum” i.e. bending forward and swinging the arms around in a circle. When ribs are sufficiently healed a larger range of motion should be attempted to increase arm flexibility.
Physical therapy is indicated in those individuals with a fractured rib who present with a compromised respiratory system, advanced age, or functional limitations associated with postural muscles.
The goal of rehabilitation is to decrease pain, prevent respiratory complications and restore function. Local application of heat or cold may provide temporary relief of discomfort, in conjunction with pharmacological treatment. There is evidence to support the use of a transcutaneous electrical nerve stimulator (TENS) for pain management in patients with uncomplicated minor rib fractures (Oncel). The physical therapist should instruct patients in deep-breathing exercises to promote full lung expansion, relieve intercostal muscle spasm, and mobilize lung secretions. Finally, shoulder and trunk gentle stretching exercises may relieve discomfort and promote chest expansion, functional shoulder mobility, and improved posture.
It is noteworthy that intensive hand, arm and leg exercises would not be the treatment of choice for a rib fracture however when someone suffers from stroke, Parkinson’s disease, Brachial plexus injury, Brain/spinal cord injuries, CP, MS or other upper and lower limb semi paresis then physical therapy solutions such as the TUTOR system come into place and can be very helpful in regaining lost movement.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR
have become a key system in neuromuscular rehabilitation and physical therapy for interactive rehabilitation exercise. These innovative devices implement an impairment based program with augmented feedback and encourage motor learning through intensive active exercises. These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. This training is customized by the occupational and physical therapist to ensure that the patient stays motivated to do intensive repetitive manual therapy and exercise practice. The TUTOR system is now part of the rehabilitation program of leading U.S. and European hospitals. Home care patients can be supported by the occupational and physical therapist offering tele-rehabilitation. See WWW.MEDITOUCH.CO.IL for further information.
About 300,000 people every year fracture their ribs in the U.S. 72% of these fractures occur in men although postmenopausal women are also prone to them due to osteoporosis. Rib fractures occur as a result of trauma such as falls and sports activities but can also come through severe coughing and even CPR treatment in older adults. A broken or fractured rib may result in internal damage to an organ, tendon or muscle. Severe damage can be done if there is a ‘flail’ chest. That is if 3 or more ribs are fractured in 2 or more places and the ribs are separated from costal cartilege or the sternum.
Earlier treatment included wrapping the chest in bandages or corsets to keep the ribs in place for healing however that is not done now as it limits proper breathing. Improper breathing can cause pneumonia and other problems.
The recommended treatment is rest, gentle exercise, pain medication and targeted physical therapy programs when the pain is less severe. Yoga and other strenuous activities are to be avoided for up to 6 weeks in most cases. Time is the main healer as the ribs heal themselves. It is recommended to take deep breaths and gentle exercises to expand the diaphragm. Sometimes even swimming 45-90 minutes per day can be helpful. Walking and moving helps to keep the airways clear and helps to prevent pneumonia and collapsed lungs.
One of the simple exercises recommended is the ”pendulum” i.e. bending forward and swinging the arms around in a circle. When ribs are sufficiently healed a larger range of motion should be attempted to increase arm flexibility.
Physical therapy is indicated in those individuals with a fractured rib who present with a compromised respiratory system, advanced age, or functional limitations associated with postural muscles.
The goal of rehabilitation is to decrease pain, prevent respiratory complications and restore function. Local application of heat or cold may provide temporary relief of discomfort, in conjunction with pharmacological treatment. There is evidence to support the use of a transcutaneous electrical nerve stimulator (TENS) for pain management in patients with uncomplicated minor rib fractures (Oncel). The physical therapist should instruct patients in deep-breathing exercises to promote full lung expansion, relieve intercostal muscle spasm, and mobilize lung secretions. Finally, shoulder and trunk gentle stretching exercises may relieve discomfort and promote chest expansion, functional shoulder mobility, and improved posture.
It is noteworthy that intensive hand, arm and leg exercises would not be the treatment of choice for a rib fracture however when someone suffers from stroke, Parkinson’s disease, Brachial plexus injury, Brain/spinal cord injuries, CP, MS or other upper and lower limb semi paresis then physical therapy solutions such as the TUTOR system come into place and can be very helpful in regaining lost movement.
The HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTORhave become a key system in neuromuscular rehabilitation and physical therapy for interactive rehabilitation exercise. These innovative devices implement an impairment based program with augmented feedback and encourage motor learning through intensive active exercises. These exercises are challenging and motivating and allow for repetitive training tailored to the patient’s performance. This training is customized by the occupational and physical therapist to ensure that the patient stays motivated to do intensive repetitive manual therapy and exercise practice. The TUTOR system is now part of the rehabilitation program of leading U.S. and European hospitals. Home care patients can be supported by the occupational and physical therapist offering tele-rehabilitation.The TUTORs are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for further information.
Wednesday, 15 August 2012
”Do Re Me Fa So La” and Physical Rehabilitation
Rehabilitation medicine combined with music therapy has been around for some time now. It as helped people with all kinds of physical disorders and even those affected by Rett syndrome. The benefits of adding music, an art, to a physical maneuver is unique and successful.Numerous studies have shown how physical therapy results are enhanced by adding music in the background or having the patient directly involved in creating the music. The music is actually ”instrumental” in physical recovery and health maintenance.
One of the beautiful benefits of using music during physical rehabilitation is that one can witness the active and consistent participation of the patient which is often not the case with standard rehabilitation. The music itself encourages participation in exercises. It can also relieve the discomfort associated with the activities. It is the goal of regular music therapy to get the participant to express himself through the music so the common goal here is to alleviate symptoms of orthopedic, pediatric and neurological conditions in order to improve range of motion, strength, communication, balance and cognition and generally the quality of life.
Occupational therapists are finding that music therapy assists clients to maximize the patient’s independence in their daily roles.
When accompanying music is used in conjunction with physical rehabilitation it would be the ultimate combination if the physical therapy products in use were of the highest quality and most efficient. Such would be the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR. These recently created devices are comfortable ergonomically designed gloves and braces that are strategically placed on affected limbs and through sensors are connected to sophisticated software. The software consists of exclusively designed games that the patient plays. Physical therapists monitor , record and evaluate the patient’s progress and design a specific exercise program for the patient. The patient himself activates the limb rather than an external robotic device that causes movement. In that way the patient has control and can progress further independently.
The TUTOR system has been in use now for some time in leading U.S. and European hospitals and rehabilitation clinics. The TUTORs are fully certified by the FDA and CE, are available for children as well as adults and can be used at the patient’s home through the use of telerehabilitation.
See WWW.MEDITOUCH.CO.IL for more information.

Tuesday, 14 August 2012
Concerns of the American Academy of Physical Medicine and Rehabilitation (AAPM&R) Vis A Vis ”Obamacare”
In 1998, a presidential commission on Consumer Protection issued a report where it defined, in its view, the purpose of a health care system. The report
stated:
“The purpose of the health care system must be to continuously reduce the impact
and burden of illness, injury, and disability, and to improve the health and
functioning of the people of the United States.”
People that have disabilities and chronic conditions depend on habilitative services
and devices. This is equivalent to the provision of antibiotics to a person who has an infection—both are
essential to medical intervention. Therefore, rehabilitative and habilitative services and devices are a
vital component of health care, especially for persons that have disabilities and chronic conditions.
These services and devices
• Speed recovery and allow discharge to one’s home sooner rather than later and
provide a higher level of function post injury or illness;
• Improve long-term health status and improve the likelihood of living independently;
• Reduce the likelihood of relapse or returning to the hospital;
• Slow or completely stop the progression of primary and secondary disabilities as they maintain functioning
and prevent further deterioration;
and
• Facilitate a return to work under appropriate circumstances.
For example, rehabilitative services and devices:
• Enable persons with spinal cord injuries to recover and regain functions through intensive
rehabilitation services ;
• Enable people who were born with congenital conditions or developmental disabilities to learn
skills and the ability to function through various therapies and assistive devices;
• Enable people with traumatic brain or spine injury to improve cognition and functioning by using
appropriate therapies and assistive devices.
It is evident from literature and personal evidence that when people withdisabilities and chronic conditions have access to treatments, including rehabilitative and habilitative
services and devices, their healthand quality of life are substantially improved. Both patients and insurers, as well the taxpayer,save many dollars of future health care costs.
The Brain Injury Association of America claims that the results of inadequate rehabilitative and habilitative services and devices for individuals with disabilities and chronic conditions to society are well known. It can result in elevated levels of medical complications, permanent disability, job loss, family dysfunction, homelessness, medical indigence, suicide and even involvement with the criminal justice system.
Inadequate treatment can also lead to lost productivity and greater utilization of public income programs and plans (such as SSI and SSDI, Medicare and Medicaid) and long-term care.
Health benefits should enable individuals to be functional, healthy and live as independently as possible. Rehabilitation services and devices should lessen the deterioration of a person’s financial status.
The AAPM&R organization is concerned that the new medical care act (Obamacare) will provide for all of the above services. One of the most efficient and cost effective recently developed physical therapy products is the TUTOR system. This is a system that will reduce the impact and burden of illness and disability. It has all the qualities of a rehabilitation program that is needed to assist patients in regaining their mobility after a stroke, brain or spinal cord injury, MS, CP, Parkinson’s disease and other upper or lower limb disabilities. The TUTOR system consists of motivating and challenging games that allow the patient to practice isolated and/or interjoint coordination exercises. Controlled exercise practice will help to prevent the development of compensatory movement patterns. The physical therapist objectively and quantitatively evaluates the treatment progress and designs a cuistomized program for the patient.
Fully certified by the FDA and CE the TUTORs (HANDTUTOR, ARMTUTOR, LEGTUTOR and 3 DTUTOR) are available for use by children as well as adults and at the patient’s home through telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Sunday, 12 August 2012
New Stroke Rehabilitation Device May Join Others Already In Use
Victoria University, New Zealand, masters student in engineering, Abigail Rajendran, 23, designed a stroke rehabilitation device and is working to market it. Rajendran believes that stroke patients will be able to rehabilitate themselves from home with the new device.
With the device strapped on to a patient’s hand the goal is to exercise it in an opening and closing motion. A connected computer game activates at the same time and keeps both sides of the brain working.
Once the patient regains the strength and can do the motion himself, he can increase the resistance with a special liquid contained in the device.
Rajendran says that until now, stroke patients had to rely on expensive and large rehabilitation equipment only found in hospitals. However this device could be used regularly at home.
Funding for a prototype has been provided by the Science and Innovation Ministry.
Few, if any, home rehabilitation instruments are available for people recovering from strokes and new technology has to be made available according to Chief executive Sunil Vather.
Apparently New Zealand stroke patients get only a few hours of therapy if they’re lucky and this device may afford them many more hours.
Miss Rajendran will present her idea in Singapore later this month, and in Brisbane in October. The device may be ready for use in about a year.
Apparently unknown to Miss Rajendran and her associates such physical therapy solutions already exist and are being used successfully in many leading U.S. and European and other hospitals and clinics. The physical therapy products known as the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR have been devised to allow intensive exercises to stroke victims as well as those afflicted with disabling Parkinson’s, MS, CP, brain/spinal cord injuries and other upper and lower limb paresis.
The TUTORs are comfortable ergonomically designed gloves and braces that are attached to the affected areas of the body and then connected to a computer that has dedicated software in the form of games. These games are played with the active initiation of the patient himself and the results are recorded and evaluated by physical therapists who then design a specific exercise program for that patient.
Since many patients have improved to the point where they no longer need hospitalization they and others who live too far from a rehabilitation clinic can avail themselves of the TUTORs at home through the use of telerehabilitation. In addition the TUTOR system is one of the most cost effective physical therapy products on the market today and they are small in relation to hospital based large equipment.
The TUTORs are fully certified by the FDA and CE. See WWW.MEDITOUCH.CO.IL for more information.

Tuesday, 7 August 2012
New Formula Predicts Rehabilitation Outcome
The journal called ”Brain” featured an article on July 31, 2012 about a development that could revolutionize rehabilitation for stoke patients. University of Auckland researchers have shown how it may be possible to predict potential recovery in stroke patients for hand and arm function. Realistic goals for recovery may be set for patients and trial outcomes for new therapies may have also have better results through this approach.
According to Professor Winston Byblow one of every six people will have a stroke at some time during their life and until now comparisons were made as to outcome based on group similarity to others with the same symptoms. An individual patient’s rehabilitation plan can not be known. ”We have developed the first clinical algorithm to actually predict the individual patient’s potential for recovery based on information gathered before rehabilitation even begins.” said Byblow.
A test is administered to the hospitalized stroke patient within 3 days of the event. It is very quick and requires no special equipment. Dr Cathy Stinear, who authored the journal article, explains that in some cases additional testing may be required such as an MRI to determine whether the pathways in the particular side of the brain remain viable and to measure the integrity of neural pathways from the brain to the arm. When the algorithm is combined with the results of the tests a prediction can be made about patient recovery at 12 weeks which is when therapy would normally end.
The information gleaned from this new test can be used to customize rehabilitation for the patient before it even begins. It is the first study to predict an individual’s potential for motor function recovery using test results obtained from that patient in the first days after stroke, according to Neurologist Professor Alan Barber, a member of the research team and Head of the Auckland Hospital Stroke Service .
The research team is now in a three year trial period of the algorithm method to show if the outcomes really benefit the patient and increases the efficiency of hospital rehabilitation services.
Once that prediction is made and actual rehabilitation commences the physical therapy product of choice may well be the HANDTUTOR and ARMTUTOR.
The HANDTUTOR and ARMTUTOR™ have been developed to allow for functional rehabilitation of the upper extremity including the shoulder,arm, elbow and wrist. The system, recommended for use for a variety of injuries and diseases including stroke, Parkinson’s, CP, MS and other upper and lower limb disabilities
, consists of an ergonomic wearable glove and arm brace together with dedicated rehabilitation software. The TUTOR systems (including the LEGTUTOR and 3DTUTOR) allow the physical and occupational therapist to report on and evaluate the patient’s functional rehabilitation progress. This allows them to prescribe the correct customized and motivating intensive exercise practice to the manual rehabilitation therapy. Intensive repetition of movement is achieved through challenging games set to the patient’s ability. The system provides detailed exercise performance instructions and precise feedback on the patient’s efforts. Controlled exercise of multijoints within the normal movement pattern prevents the development of undesired and compensatory joint movement and ensures better performance of functional tasks. Telerehabilitation allows the recovering patient to continue his physical therapy at home. The system is used by many leading rehabilitation centers worldwide and has full FDA and CE certification. See WWW.MEDITOUCH.CO.IL for more information.

Thursday, 2 August 2012
Finding Solutions for Pediatric Physiotherapy
Canada is one of the most beautiful and advamced countries in the world. It has a stereotype reputation of perfection around the world. However it, like many other governments has to watch it’s financial pocketbook. Probably that’s why the province of Ontario has a quirky rule that children with spinal cord injuries aren’t entitled to certain medical treatments.
One such case is that of Ben Wood who spends hours each week retraining his legs, hoping to be able to take a few more steps. His family worries about where the money will come to pay for this intensive physiotherapy.
Since ben is only 17 Ontario does not cover this type of physiotherapy because he is under the age of 18, as the ”Star’s” Barbara Turnbull reported on July 30, 2012.
Apparently even Ontario’s health minister can’t explain why the province pays for out-patient rehab services for adults that have spinal cord injuries but not for children.
Intensive therapy for young people with incomplete spinal cord injuries – like Wood – have the best potential for improvement of their condition through intensive therapy simply because their brains are capable of forming new neural pathways. Young people can gain the most from potential mobility increases. There is a difference between being wheelchair bound or being able to stand and take a few steps. It can mean being independent, having more job opportunities and achieving a better future.
In some cases the results of specialized neurological intensive therapy have been very dramatic. Nick Schoenhoff had a spinal cord injury in a snowboard accident when he was just 13. He went home from the rehab hospital in a wheelchair and was told that there was nothing else to be done. However, after years of intensive physiotherapy which was funded privately and through community donations, Schoenhoff became a university student who only uses a wheelchair for long distances. He uses a cane the rest of the time.
His family actually started a fund called ”Support in Motion”, to help provide similar therapy for other Ontario teens like Wood. It’s wonderful that this family is doing this to help others, but shouldn’t the province be providing these services?
The health minister, Deb Matthews, said that she’s looking into how to incorporate these services.
One of the solutions to providing physical therapy for spinal cord injuries that is most cost effective and is available for children as young as 5 is the TUTOR system. Consisting of the HANDTUTOR, ARMTUTOR, LEGTUTOR and 3DTUTOR these physical therapy products were created to accommodate the need for intensive exercises suffered by patients that experienced not only spinal cord injuries but also brain injuries, strokes, Parkinson’s disease, CP, MS and other kinds of upper and lower limb disabilities.
The TUTOR system consists of wearable ergonomically designed devices together with powerful dedicated rehabilitation software. It consists of motivating and challengoing games that allow the patient to practice isolated and/or interjoint coordination exercises. The dedicated software allows the physical therapist to fully customize the exercises to the patient’s movement ability. In addition the therapist can objectively and quantitatively evaluate and report on the treatment progres. The TUTOR system optimizes the patient’s motor, sensory and cognitive performance and allows the patient to better perform everyday functional tasks to improve their quality of life.
The TUTORs are fully certified by the FDA and CE and can be used in the patient’s home via telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Wednesday, 1 August 2012
Is Knee Surgery Really Needed?
The web is full of articles about knee surgery and how more and more people are opting for this painful solution to osteoarthritis. However a study recently concluded that there may be a way to avoid such an operation completely.
A study was conducted in a large military hospital in Texas recently indicating that physical therapy consisting of manual therapy, stretching and strengthening as an exercise regimen may help people with osteoarthritis of the knee avoid a knee joint replacement surgery.
During the study, 83 patients with osteoarthritis of the knee were randomly assigned to two groups.The first group of 42 patients received treatment consisting of manual therapy and therapeutic exercise twice a week for four weeks.The second group of 41 patients received a placebo treatment where they received ultrasound in a dosage far below a therapeutic level. The mean age of the partipants was 60 and 62 years respectively.
Results were measured at four weeks, eight weeks, and one year post-treatment. The study reports that “Clinically and statistically significant improvements were observed in the treatment group but not in the placebo group”.
The study also reports that “the average distance walked in the treatment group was 170 more than that in the placebo group. At one year, patients in the treatment group had clinically and statistically significant gains over baseline in walking distance. While 20 percent of patients in the placebo group had undergone knee arthroplasty, only 5 percent of patients in the treatment group had.”
The study concluded with a statement saying “In patients with osteoarthritis of the knee, a combination of manual physical therapy and stretching, range-of-motion, and strengthening exercises may yield improvements in functional ability as well as in subjective measures of pain, stiffness, and function and may delay or prevent the need for surgical intervention. These improvements may persist well after the conclusion of clinical treatment.”
When physical exercise is indicated for a problematic knee due to osteoarthritis one of the most effective physical therapy solutions is the LEGTUTOR. The LEGTUTOR consists of a safe comfortable leg brace with position sensors that precisely record three dimensional (3D) hip and knee movements.The LEGTUTOR has a range of motion limiter that can limit the dynamic range of knee extension and flexion. Rehabilitation games allow the patient to exercise Range of Motion (ROM), speed and accuracy of movement. The LEGTUTOR facilitates evaluation and treatment of the lower extremity including isolated and combined hip and knee movements.
The LEGTUTOR and its sister physical therapy products (HANDTUTOR, ARMTUTOR and 3DTUTOR) are one of the most cost effective medical devices available for what it accomplishes. Currently in use in leading U.S. and European hospitals and clinics the TUTOR system is fully certified by the FDA and CE and can be used by children as well as adults. They are also available for use in the patient’s home via telerehabilitation. See WWW.MEDITOUCH.CO.IL for more information.

Subscribe to:
Posts (Atom)